I Olivier Chabot will have an ApoB of 0.9 g/L or less by December 1st 2024.
I have written the sentence above three times every morning since July 11th, 2024.
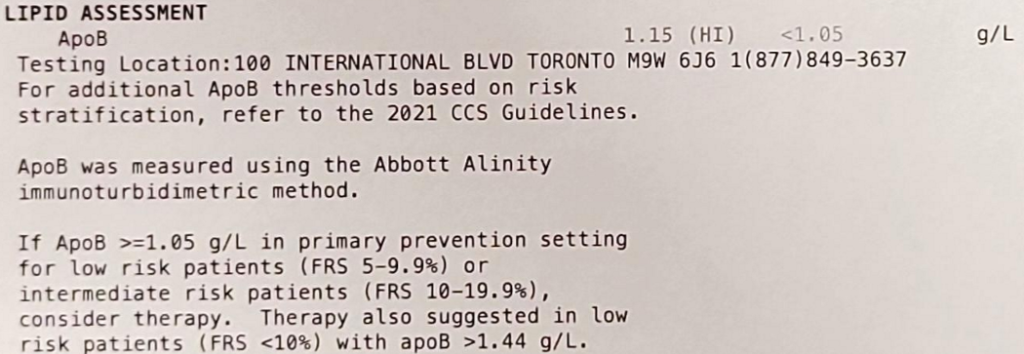
On June 25th 2024, a blood test revealed ApoB levels of 1.15 g/L which is considered high and increases the risk of heart disease. I’m 28 years old, active and eat relatively well. It was a shock to me.
After reading Peter Attia’s book on longevity, Outlive, I know we want to lower apoB as much as possible and as early as possible. My doctor’s software could not calculate the ten-year risk score because I needed to be at least 30 years old. He still offered to prescribe cholesterol-lowering medication, but I wanted to try a behavioural/nutritional intervention first.
My plan was to :
- Write the sentence three times each morning to remind me of my goal and to prime my subconscious to make healthier decisions throughout the day.
- Take Metamucil capsules daily. I’ve been taking 5 capsules twice per day. Sometimes I opt for the liquid version. Psyllium fibre supposedly helps curb appetite, maintain healthy blood sugar levels and lower cholesterol. Subjectively, I can attest to the appetite reduction. I’ve been tracking my weight, so it’ll be interesting to see if my body composition changes in the next few months.
- Order healthier options when we go to restaurants. This is a low-hanging fruit to clean up food intake. It’s still exciting to try new delicious bowls and salads.
Of course, the manifestation exercise itself is not likely to directly cause lower apoB levels. However, I’m curious to see whether psyllium husk and dietary modifications will be enough to lower apoB levels. Taking Metamucil is somewhat annoying and expensive. To lower cholesterol, they recommend taking five capsules four times per day. That’s approximately 4$ per day or 1500$ per year. A cholesterol-lowering drug is likely to be cheaper, more convenient to ingest, and more effective at lowering apoB. Hence, I’ll likely experiment with Crestor to lower apoB as much as possible when I meet with my doctor this winter after another blood test. Stay posted for an update.
Peter Attia Outlive Notes from my Book Summary
- “Eating lots of saturated fat can increase levels of atherosclerosis-causing lipoproteins in blood, but most of the actual cholesterol that we consume in our food ends up being excreted out our backsides. The vast majority of the cholesterol in our circulation is actually produced by our own cells.”
- ““There’s no connection whatsoever between cholesterol in food and cholesterol in blood,” Keys said in a 1997 interview. “None. And we’ve known that all along. Cholesterol in the diet doesn’t matter at all unless you happen to be a chicken or a rabbit.” It took nearly two more decades before the advisory committee responsible for the US government dietary guidelines finally conceded (in 2015) that “cholesterol is not a nutrient of concern for overconsumption.” Glad we settled that.”
- “evidence has piled up pointing to apoB as far more predictive of cardiovascular disease than simply LDL-C, the standard “bad cholesterol” measure. According to an analysis published in JAMA Cardiology in 2021, each standard-deviation increase in apoB raises the risk of myocardial infarction by 38 percent in patients without a history of cardiac events or a diagnosis of cardiovascular disease (i.e., primary prevention). That’s a powerful correlation.”
- “I have all my patients tested for apoB regularly, and you should ask for the same test the next time you see your doctor. (Don’t be waved off by nonsensical arguments about “cost”: It’s about twenty to thirty dollars.)”
- “In my clinical experience, about a third to half of people who consume high amounts of saturated fats (which sometimes goes hand in hand with a ketogenic diet) will experience a dramatic increase in apoB particles, which we obviously don’t want.[*8] Monounsaturated fats, found in high quantities in extra virgin olive oil, macadamia nuts, and avocados (among other foods), do not have this effect, so I tend to push my patients to consume more of these, up to about 60 percent of total fat intake. The point is not necessarily to limit fat overall but to shift to fats that promote a better lipid profile.”
- “Simply put, I think you can’t lower apoB and LDL-C too much, provided there are no side effects from treatment. You want it as low as possible.”
- “Once you understand that apoB particles—LDL, VLDL, Lp(a)—are causally linked to ASCVD, the game completely changes. The only way to stop the disease is to remove the cause, and the best time to do that is now.”
- “But for many patients, if not for most, lowering apoB to the levels we aim for—the physiologic levels found in children—cannot be accomplished with diet alone, so we need to use nutritional interventions in tandem with drugs.”
- “While there are seven statins on the market, I tend to start with rosuvastatin (Crestor) and only pivot from that if there is some negative effect from the drug (e.g., a symptom or biomarker).”
- “Another way to think of all this is that someone might be considered “low risk” at a given point—but on what time horizon? The standard is ten years. But what if our time horizon is “the rest of your life”?”
- “We know that smoking is causally linked to lung cancer. Should we tell someone to stop smoking only after their ten-year risk of lung cancer reaches a certain threshold?”