 Outlive: The Science and Art of Longevity by Peter Attia MD
Outlive: The Science and Art of Longevity by Peter Attia MDMy rating: 5 of 5 stars
Solid evidence-based book on longevity. That said, the first section on tactics/strategy and the last chapter on emotions were my personal favourite. This book has many pearls and will help me extend my lifespan and health span by a few years. However, I think the true value of this book lies in empowering the reader to think about and take their life seriously.
View all my reviews
TLDR – Main Takeaways
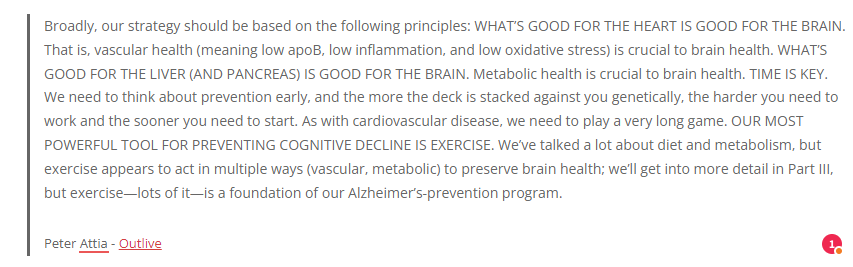
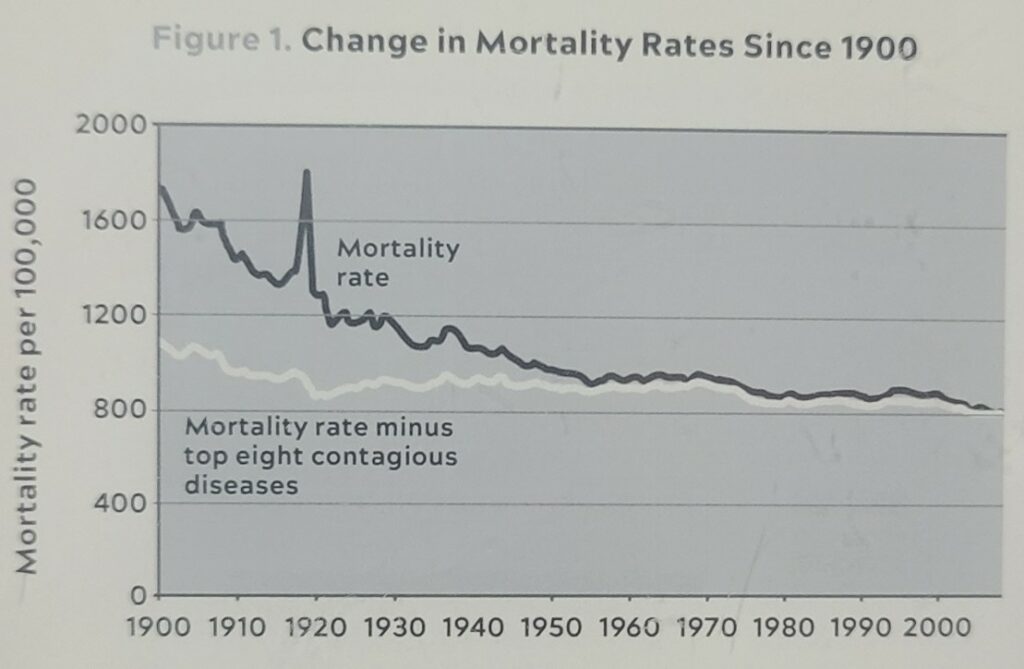
- Medicine 2.0 has made tremendous progress in limiting fast deaths, but relatively little in preventing slow deaths. We need Medicine 3.0 to extend healthspan until the very last drops of lifespan (see curves below).
- Everybody should be training for the centenarian decathlon. Not only do we want to live to 100, but we need to be functional in our later years. We can reverse engineer the math to figure out how much we need to train to accomplish our goal.
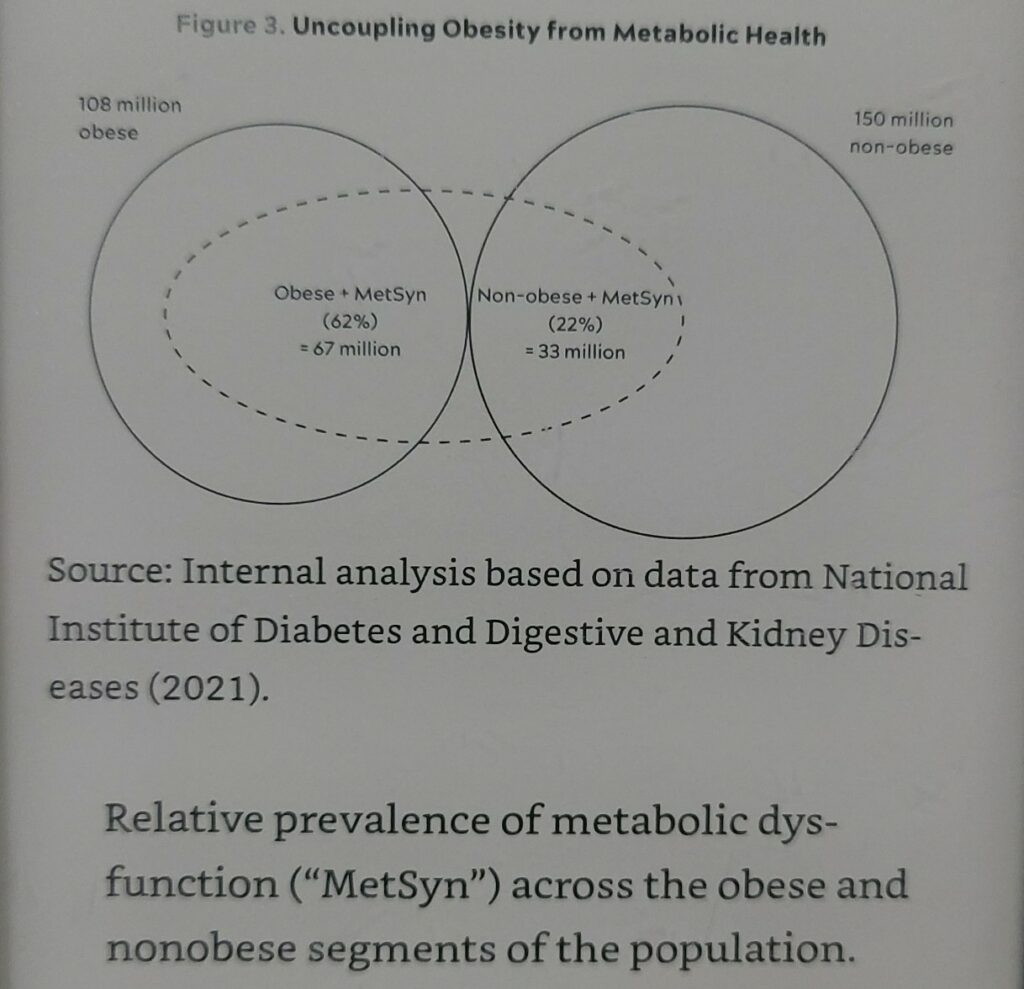
- Obesity is not a sufficient cause of metabolic syndrome (see chart below).
- Don’t wait to be diagnosed with a disease. Most if not all horsemen start many decades before symptoms appears. Now is the best time to start your prevention plan.
- “”Another way to think of all this is that someone might be considered “low risk” at a given point—but on what time horizon? The standard is ten years. But what if our time horizon is “the rest of your life”?””
- “Tactics without strategy is the noise before defeat.” – Sun Tzu
- Exercise trumps every other intervention to extend lifespan. But more importantly, done properly, it certainly extends healthspan.
- Losing a couple of years of life at the tail end is a worthwhile tradeoff if your healthspan is extended by decades.
- Nutrition is tricky. Don’t get caught in the nitty-gritty in all the tactics and genes. Remember that the goal is the live a more fulfilling life for longer.
- “Why would you want to live longer if you’re so unhappy?” – Esther Perel
Book Notes & Highlights
Introduction
In short, it had finally dawned on me that the only way to solve the problem was not to get better at catching the eggs. Instead, we needed to try to stop the guy who was throwing them. We had to figure out how to get to the top of the building, find the guy, and take him out.
Peter Attia – Outlive
There comes a point where we need to stop just pulling people out of the river. We need to go upstream and find out why they’re falling in.
Bishop Desmond Tutu
Part I
Chapter 1 – The Long Game
The Chronology of Death
- “Later, as a surgical resident at Johns Hopkins, I would learn that death comes at two speeds: fast and slow.”
- “Medicine’s biggest failing is in attempting to treat all these conditions at the wrong end of the timescale—after they are entrenched—rather than before they take root.”
The Two Components of Longevity
- “I hope to convince you that with enough time and effort, you can potentially extend your lifespan by a decade and your healthspan possibly by two, meaning you might hope to function like someone twenty years younger than you.”
- “The other key point is that lifespan and healthspan are not independent variables; they are tightly intertwined.”
Chapter 2 – Medicine 3.0
The time to repair the roof is when the sun is shining.
John F. Kennedy
When did Noah build the ark? Long before it began to rain.
Peter Attia – Outlive
Medicine 2.0 tries to figure out how to get dry after it starts raining. Medicine 3.0 studies meteorology and tries to determine whether we need to build a better roof, or a boat.
Peter Attia – Outlive
| Medicine 2.0 | Medicine 3.0 | |
| Emphasis | Treatment of symptoms | Proactive prevention of disease |
| Treats patients as | The average patient | A nuanced individual |
| Risk | Avoid at all costs | Assesses risk of action and non-action carefully |
| Focus | Extending lifespan | Extending healthspan |
| Patient is | Passive with no responsibility and agency | Active with responsibility and agency |
| Tactics | Procedures (surgery) and medications | Exercise, nutrition, sleep, emotional health, and exogenous molecules (drugs, hormones, supplements) |
First, Do No Harm
- “The trouble began with Hippocrates. Most people are familiar with the ancient Greek’s famous dictum: “First, do no harm.” It succinctly states the physician’s primary responsibility, which is to not kill our patients or do anything that might make their condition worse instead of better. Makes sense. There are only three problems with this: (a) Hippocrates never actually said these words,[*1] (b) it’s sanctimonious bullshit, and (c) it’s unhelpful on multiple levels.”
- “What bothers me most about “First, do no harm,” though, is its implication that the best treatment option is always the one with the least immediate downside risk—and, very often, doing nothing at all. Every doctor worth their diploma has a story to disprove this nonsense.”
- “My point is that a physician who has never done any harm, or at least confronted the risk of harm, has probably never done much of anything to help a patient either. And as in the case of my teenage stabbing victim, sometimes doing nothing is the riskiest choice of all.”
The Financial Case for Medicine 3.0
- “There are few insurance reimbursement codes for most of the largely preventive interventions that I believe are necessary to extend lifespan and healthspan. Health insurance companies won’t pay a doctor very much to tell a patient to change the way he eats, or to monitor his blood glucose levels in order to help prevent him from developing type 2 diabetes. Yet insurance will pay for this same patient’s (very expensive) insulin after he has been diagnosed.”
- “Nearly all the money flows to treatment rather than prevention—and when I say “prevention,” I mean prevention of human suffering.”
- “Continuing to ignore healthspan, as we’ve been doing, not only condemns people to a sick and miserable older age but is guaranteed to bankrupt us eventually.”
Chapter 3 – Objective, Strategy, Tactics
Strategy without tactics is the slowest route to victory. Tactics without strategy is the noise before defeat.
Sun Tzu
Our Objective
- “To delay death, and to get the most out of our extra years.”
- “We want to delay or prevent these conditions so that we can live longer without disease, rather than lingering with disease.”
Strategy versus Tactic
- “To achieve our objectives, we first need to have a strategy: an overall approach, a conceptual scaffolding or mental model that is informed by science, is tailored to our goals, and gives us options. Our specific tactics flow from our strategy, and the strategy derives from our objective.”
- “The point is that the tactics are what you do when you are actually in the ring. The strategy is the harder part, because it requires careful study of one’s opponent, identifying his strengths and weaknesses, and figuring out how to use both to your advantage, well before actually stepping in the ring.”
- “Of course, not every problem you face requires a strategy. In fact, many don’t. You don’t need a strategy if your objective is, say, to avoid getting a sunburn.”
- “Without an understanding of the strategy, and the science that informs it, our tactics will not mean much, and you’ll forever ride the merry-go-round of fad diets and trendy workouts and miracle supplements.”
- “A good strategy allows us to adopt new tactics and discard old ones in service of our objectives.”
- “In a sense it’s a bit like charting an investment strategy: we are seeking the tactics that are likeliest, based on what we know now, to deliver a better-than-average return on our capital, while operating within our own individual tolerance for risk.”
The Healthspan 3D Space
- “I think about healthspan and its deterioration in terms of three categories, or vectors. The first vector of deterioration is cognitive decline. … The second vector of deterioration is the decline and eventual loss of function of our physical body. … The third and final category of deterioration, I believe, has to do with emotional health. Unlike the others, this one is largely independent of age…”
- “Why would you want to live longer if you’re so unhappy?” – Esther Perel
The Weakness of Evidence-based Medicine
- “These trials take heterogeneous inputs (the people in the study or studies) and come up with homogeneous results (the average result across all those people). Evidence-based medicine then insists that we apply those average findings back to individuals. The problem is that no patient is strictly average.”
- Waiting for perfect studies (which are sometimes impossible to conduct with humans) puts us at risk of the harm of doing nothing.
Evidence-informed, Risk-adjusted Precision Medicine
- “The purists of evidence-based medicine demand data from randomized controlled trials (RCTs) before doing anything.”
- “The best we can hope for is reducing our uncertainty. A good experiment in biology only increases or decreases our confidence in the probability that our hypothesis is true or false.”
- “Our Option B strategy is based on combining insights from five different sources of data that, viewed separately, probably aren’t strong enough to act on. When taken together, however, they can provide a solid foundation for our tactics. But our supporting framework must shift, from exclusively evidence-based to evidence-informed, risk-adjusted precision medicine.”
- Centenarian Studies
- Limitation: “Observational rather than experimental, so we can’t truly infer cause and effect.”
- Animal “Models”
- “My rule of thumb is that if a given intervention can be shown to extend lifespan or healthspan in multiple species spanning a billion years of evolution, for example, from worms to monkeys, then I am inclined to take it seriously.”
- Human Studies of the Horsemen.
- Molecular & Mechanistic Insights
- Mendelian Randomization (MR for short)
- MR helps bridge the gap between randomized controlled trials, which can establish causality, and pure epidemiology, which often cannot.”
- “It accomplishes this by letting nature do the randomization.[*2] By considering the random variation in relevant genes and comparing them against the observed results, it eliminates many of the biases and confounders that limit the usefulness of pure epidemiology.”
Our Strategy
- “I used to prioritize nutrition over everything else, but I now consider exercise to be the most potent longevity “drug” in our arsenal, in terms of lifespan and healthspan. The data are unambiguous: exercise not only delays actual death but also prevents both cognitive and physical decline, better than any other intervention.”
- “The best science out there says that what you eat matters, but the first-order term is how much you eat: how many calories you take into your body.”
- “On Wall Street, gaining an advantage like this is called alpha, and we’re going to borrow the idea and apply it to health. I propose that with some unorthodox but very reasonable lifestyle changes, you can minimize the most serious threats to your lifespan and healthspan and achieve your own measure of longevity alpha.”
Part II
Chapter 4 – Centenarians
Centenarians
- “More broadly, it’s worth asking: What do healthy centenarians actually have in common? And, more importantly, what can we learn from them—if anything? Do they really live longer because of their idiosyncratic behaviors, like drinking whiskey, or despite them? Is there some other common factor that explains their extreme longevity, or is it simply luck?”
- “Centenarians are no more health-conscious than the rest of us. They may actually be worse.”
The Death Lottery
- There’s always a chance of dying at any moment. Are centenarians simply the ones getting lucky and escaping death every year, like the monkey flipping 100 heads in a row?
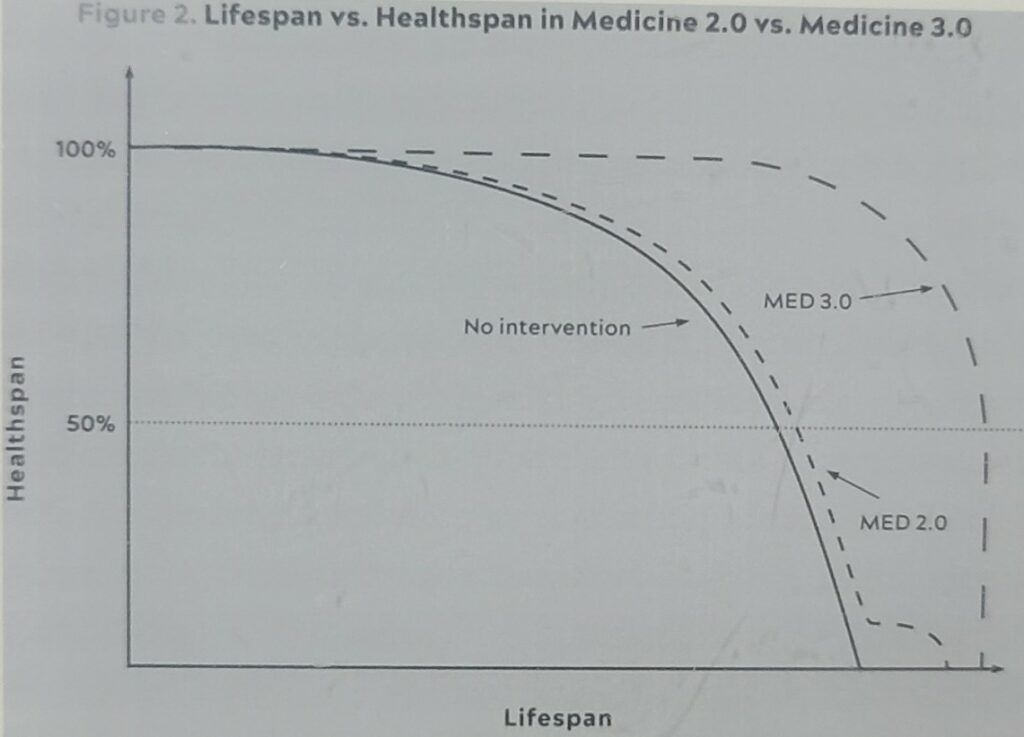
- “The overall mortality rate for Americans ages 100 and older is a staggering 36 percent, meaning that if Grandma is 101, she has about a one-in-three chance of dying in the next twelve months.”
The Genetic Lottery
While your genome is immutable, at least for the near future, gene expression can be influenced by your environment and your behaviors.
Peter Attia – Outlive
- “Broader genetic studies suggest that hundreds, if not thousands, of genes could be involved, each making its own small contribution—and that there is no such thing as a “perfect” centenarian genome.”
- “Thus it appears that no two centenarians follow the exact same genetic path to reaching extreme old age. There are many ways to achieve longevity; not just one or two.”
- “Studies of Scandinavian twins have found that genes may be responsible for only about 20 to 30 percent of the overall variation in human lifespan. The catch is that the older you get, the more genes start to matter.”
- “These individuals appeared to have very little in common with one another genetically. And their longevity may be due to dumb luck after all.”
- “One of the most potent individual genes yet discovered is related to cholesterol metabolism, glucose metabolism—and Alzheimer’s disease risk. You may have heard of this gene, which is called APOE, because of its known effect on Alzheimer’s disease risk.”
- “The e2 variant of APOE, on the other hand, seems to protect its carriers against dementia—and it also turns out to be very highly associated with longevity.”
- “Researchers have identified two other cholesterol-related genes, known as CETP and APOC3, that are also correlated with extreme longevity (and may explain why centenarians rarely die from heart disease).”
- “These are variants in a particular gene called FOXO3 that seem to be directly relevant to human longevity.”
- “Here’s where we start to see some hope, because FOXO3 can be activated or suppressed by our own behaviors. For example, when we are slightly deprived of nutrients, or when we are exercising, FOXO3 tends to be more activated, which is what we want.”
Genetactics
- “Can we, through our behaviors, somehow reap the same benefits that centenarians get for “free” via their genes? Or to put it more technically, can we mimic the centenarians’ phenotype, the physical traits that enable them to resist disease and survive for so long, even if we lack their genotype? Is it possible to outlive our own life expectancy if we are smart and strategic and deliberate about it? If the answer to this question is yes, as I believe it is, then understanding the inner workings of these actuarial lottery winners—how they achieve their extreme longevity—is a worthwhile endeavor that can inform our strategy.”
- “Put another way, if we want to outlive our life expectancy and live better longer, we will have to work hard to earn it—through small, incremental changes.”
- “Curiously, despite the fact that female centenarians outnumber males by at least four to one, the men generally scored higher on both cognitive and functional tests.”
Chapter 5 – Eat Less, Live Longer?
Longevity Drugs
- “But rapamycin turned out to be so much more than the next Dr. Scholl’s foot spray. It proved to have powerful effects on the immune system, and in 1999 it was approved by the US Food and Drug Administration (FDA) to help transplant patients accept their new organs.”
- “The reason rapamycin has so many diverse applications is thanks to a property that Sehgal had observed, but never explored, which is that it tends to slow down the process of cellular growth and division.”
- “Why do we care about mTOR? Because this mechanism turns out to be one of the most important mediators of longevity at the cellular level. Not only that, but it is highly “conserved,” meaning it is found in virtually all forms of life, ranging from yeast to flies to worms and right on up to us humans. In biology, “conserved” means that something has been passed on via natural selection, across multiple species and classes of organisms—a sign that evolution has deemed it to be very important.”
- “Kaeberlein has also observed that rapamycin seems to reduce systemic inflammation, perhaps by tamping down the activity of so-called senescent cells, which are “older” cells that have stopped dividing but have not died; these cells secrete a toxic cocktail of inflammatory cytokines, chemicals that can harm surrounding cells. Rapamycin seems to reduce these inflammatory cytokines.”
- “Even though the drug had been given late in life, when the mice were already “old” (six hundred days, roughly the equivalent of humans in their sixties), it had still boosted the animals’ remaining life expectancy by 28 percent for males and 38 percent for females. It was the equivalent of a pill that could make a sixty-year-old woman live to the age of ninety-five.”
- “The real headline here, however, was that no other molecule had been shown to extend lifespan in a mammal. Ever.“
- Nicotinamide riboside (NR) & Resveratrol did not have robust effects on lifespan.
- “Of course, there are no data showing that any of these supplements lengthen life or improve health in humans.”
- “This study suggested that rapamycin (and its derivatives) might actually be more of an immune modulator than an “immunosuppressor,” as it had almost always been described before this study: that is, under some dosing regimens it can enhance immunity, while under completely different dosing regimens it may inhibit immunity.”
- “Giving the drug daily, as is typically done with transplant patients, appears to inhibit both complexes, while dosing the drug briefly or cyclically inhibits mainly mTORC1, unlocking its longevity-related benefits, with fewer unwanted side effects.”
- “A small but growing number of people, including me and a handful of my patients, already take rapamycin off-label for its potential geroprotective benefits. I can’t speak for everyone, but taking it cyclically does appear to reduce unwanted side effects, in my experience.”
- “Over time, researchers noticed (and studies appeared to confirm) that patients on metformin appeared to have a lower incidence of cancer than the general population. One large 2014 analysis seemed to show that diabetics on metformin actually lived longer than nondiabetics, which is striking. But none of these observations “prove” that metformin is geroprotective—hence the need for a clinical trial.”
Caloric Restriction (CR)
- “CR seems to improve their healthspan in addition to their lifespan. You’d think that hunger might be unhealthy, but the scientists have actually found that the less they feed the animals, the longer they live. Its effects seem to be dose dependent, up to a point, almost like a drug.”
- “Reducing the amount of nutrients available to a cell seems to trigger a group of innate pathways that enhance the cell’s stress resistance and metabolic efficiency—all of them related, in some way, to mTOR.”
- “Specifically, it seems to be a drop in amino acids that induces mTOR to shut down, and with it all the anabolic (growth) processes that mTOR controls. Instead of making new proteins and undergoing cell division, the cell goes into a more fuel-efficient and stress-resistant mode, activating an important cellular recycling process called autophagy, which means “self-eating” (or better yet, “self-devouring”).”
- “Impaired autophagy is thought to be an important driver of numerous aging-related phenotypes and ailments, such as neurodegeneration and osteoarthritis. Thus, I find it fascinating that this very important cellular mechanism can be triggered by certain kinds of interventions, such as a temporary reduction in nutrients (as when we are exercising or fasting)—and the drug rapamycin.”
- “For one, CR’s usefulness remains doubtful outside of the lab; very lean animals may be more susceptible to death from infection or cold temperatures. And while eating a bit less worked for Luigi Cornaro, as well as for some of my own patients, long-term severe caloric restriction is difficult if not impossible for most humans to sustain. Furthermore, there is no evidence that extreme CR would truly maximize the longevity function in an organism as complex as we humans, who live in a more variable environment than the animals described above. While it seems likely that it would reduce the risk of succumbing to at least some of the Horsemen, it seems equally likely that the uptick in mortality due to infections, trauma, and frailty might offset those gains.”
Chapter 6 – The Crisis of Abundance
Nonalcoholic Fatty Liver Disease (NAFLD)
- “More than one in four people on this planet have some degree of NASH or its precursor, known as nonalcoholic fatty liver disease, or NAFLD, which is what we had observed in our patient that day in the operating room.”
- “NAFLD is highly correlated with both obesity and hyperlipidemia (excessive cholesterol), yet it often flies under the radar, especially in its early stages.”
- NAFLD ==> NASH ==> Type 2 Diabetes
- “NAFLD and NASH are basically two stages of the same disease. NAFLD is the first stage, caused by (in short) more fat entering the liver or being produced there than exiting it. The next step down the metabolic gangplank is NASH, which is basically NAFLD plus inflammation, similar to hepatitis but without a viral infection.”
- “Type 2 diabetes is technically a distinct disease, defined very clearly by glucose metrics, but I view it as simply the last stop on a railway line passing through several other stations, including hyperinsulinemia, prediabetes, and NAFLD/NASH. If you find yourself anywhere on this train line, even in the early stages of NAFLD, you are likely also en route to one or more of the other three Horsemen diseases (cardiovascular disease, cancer, and Alzheimer’s disease).”
- “Both NAFLD and NASH are still reversible.”
- “The liver is a highly resilient organ, almost miraculously so. It may be the most regenerative organ in the human body. When a healthy person donates a portion of their liver, both donor and recipient end up with an almost full-sized, fully functional liver within about eight weeks of the surgery, and the majority of that growth takes place in just the first two weeks.”
“Nature is quite happy for us to be fat and frankly doesn’t care if we get diabetes.”
PETER ATTIA – OUTLIVE
Obesity
- “In the late 1970s, the average American adult male weighed 173 pounds. Now the average American man tips the scale at nearly 200 pounds. In the 1970s, a 200-pound man would have been considered very overweight; today he is merely average. So you can see how in the twenty-first century, “average” is not necessarily optimal.”
- “Obesity is merely one symptom of an underlying metabolic derangement, such as hyperinsulinemia, that also happens to cause us to gain weight.”
- “But not everyone who is obese is metabolically unhealthy, and not everyone who is metabolically unhealthy is obese.”
- “Studies have found that approximately one-third of those folks who are obese by BMI are actually metabolically healthy, by many of the same parameters used to define the metabolic syndrome (blood pressure, triglycerides, cholesterol, and fasting glucose, among others). At the same time, some studies have found that between 20 and 40 percent of nonobese adults may be metabolically unhealthy, by those same measures.”
Metabolic Syndrome
- “Today we call this cluster of problems “metabolic syndrome” (or MetSyn), and it is defined in terms of the following five criteria:
- High blood pressure (>130/85)
- High triglycerides (>150 mg/dL)
- Low HDL cholesterol (<40 mg/dL in men or <50 mg/dL in women)
- Central adiposity (waist circumference >40 inches in men or >35 in women)
- Elevated fasting glucose (>110 mg/dL)
- If you meet three or more of these criteria, then you have the metabolic syndrome.”
- “Metabolism is the process by which we take in nutrients and break them down for use in the body.”
- “One reason I find value in the concept of metabolic syndrome is that it helps us see these disorders as part of a continuum and not a single, binary condition. Its five relatively simple criteria are useful for predicting risk at the population level.”
- “In my patients, I monitor several biomarkers related to metabolism, keeping a watchful eye for things like elevated uric acid, elevated homocysteine, chronic inflammation, and even mildly elevated ALT liver enzymes. Lipoproteins, which we will discuss in detail in the next chapter, are also important, especially triglycerides; I watch the ratio of triglycerides to HDL cholesterol (it should be less than 2:1 or better yet, less than 1:1), as well as levels of VLDL, a lipoprotein that carries triglycerides—all of which may show up many years before a patient would meet the textbook definition of metabolic syndrome.”
- “But the first thing I look for, the canary in the coal mine of metabolic disorder, is elevated insulin.”
Safe Energy Storage
- “Consider that five grams of glucose, spread out across one’s entire circulatory system, is normal, while seven grams—a teaspoon and a half—means you have diabetes. As I said, the liver is an amazing organ.”
- “Even a relatively lean adult may carry ten kilograms of fat in their body, representing a whopping ninety thousand calories of stored energy.”
- “The twist here is that fat—that is, subcutaneous fat, the layer of fat just beneath our skin—is actually the safest place to store excess energy. Fat in and of itself is not bad. It’s where we should put surplus calories. That’s how we evolved.”
- “This fat flux goes on continually, and as long as you haven’t exceeded your own fat storage capacity, things are pretty much fine.”
- “As more calories flood into your subcutaneous fat tissue, it eventually reaches capacity and the surplus begins spilling over into other areas of your body: into your blood, as excess triglycerides; into your liver, contributing to NAFLD; into your muscle tissue, contributing directly to insulin resistance in the muscle (as we’ll see); and even around your heart and your pancreas (figure 4). None of these, obviously, are ideal places for fat to collect; NAFLD is just one of many undesirable consequences of this fat spillover.”
- “All other things being equal, someone who carries a bit of body fat may also have greater fat-storage capacity, and thus more metabolic leeway than someone who appears to be more lean.”
- “This is why I insist my patients undergo a DEXA scan annually—and I am far more interested in their visceral fat than their total body fat.”
Insulin Resistance
- “Insulin resistance is a term that we hear a lot, but what does it really mean? Technically, it means that cells, initially muscle cells, have stopped listening to insulin’s signals, but another way to visualize it is to imagine the cell as a balloon being blown up with air. Eventually, the balloon expands to the point where it gets more difficult to force more air inside. You have to blow harder and harder. This is where insulin comes in, to help facilitate the process of blowing air into the balloon. The pancreas begins to secrete even more insulin, to try to remove excess glucose from the bloodstream and cram it into cells. For the time being it works, and blood glucose levels remain normal, but eventually you reach a limit where the “balloon” (cells) cannot accept any more “air” (glucose).”
- “Insulin is all about fat storage, not fat utilization.”
- “In 1940 the famed diabetologist Elliott Joslin estimated that about one person in every three to four hundred was diabetic, representing an enormous increase from just a few decades earlier, but it was still relatively uncommon. By 1970, around the time I was born, its prevalence was up to one in every fifty people. Today over 11 percent of the US adult population, one in nine, has clinical type 2 diabetes, according to a 2022 CDC report, including more than 29 percent of adults over age sixty-five. Another 38 percent of US adults—more than one in three—meet at least one of the criteria for prediabetes. That means that nearly half of the population is either on the road to type 2 diabetes or already there.”
- “But the first thing I look for, the canary in the coal mine of metabolic disorder, is elevated insulin.”
- “One test that I like to give patients is the oral glucose tolerance test, or OGTT, where the patient swallows ten ounces of a sickly-sweet, almost undrinkable beverage called Glucola that contains seventy-five grams of pure glucose, or about twice as much sugar as in a regular Coca-Cola.[*6] We then measure the patient’s glucose and their insulin, every thirty minutes over the next two hours.”
- “But the insulin in someone at the early stages of insulin resistance will rise very dramatically in the first thirty minutes and then remain elevated, or even rise further, over the next hour. This postprandial insulin spike is one of the biggest early warning signs that all is not well.”
- “Studies have found that insulin resistance itself is associated with huge increases in one’s risk of cancer (up to twelvefold), Alzheimer’s disease (fivefold), and death from cardiovascular disease (almost sixfold)—all of which underscores why addressing, and ideally preventing, metabolic dysfunction is a cornerstone of my approach to longevity.”
Fructose
- “But as it turns out, we humans have a unique capacity for turning calories from fructose into fat.”
- “At some point, our primate ancestors underwent a random genetic mutation that effectively switched on their ability to turn fructose into fat: the gene for the uricase enzyme was “silenced,” or lost. Now, when these apes consumed fructose, they generated lots of uric acid, which caused them to store many more of those fructose calories as fat.”
- “Whatever form it takes, fructose does not pose a problem when consumed the way that our ancestors did, before sugar became a ubiquitous commodity: mostly in the form of actual fruit. It is very difficult to get fat from eating too many apples, for example, because the fructose in the apple enters our system relatively slowly, mixed with fiber and water, and our gut and our metabolism can handle it normally.”
- “I test my patients’ levels of uric acid, not only because high levels may promote fat storage but also because it is linked to high blood pressure. High uric acid is an early warning sign that we need to address a patient’s metabolic health, their diet, or both.”
- “I’ve seen patients work themselves into NAFLD by drinking too many “healthy” fruit smoothies, for the same reason: they are taking in too much fructose, too quickly.”
- “While it may be in vogue to vilify high-fructose corn syrup, which is 55 percent fructose and 45 percent glucose, it’s worth pointing out that good old table sugar (sucrose) is about the same, consisting of 50 percent fructose and 50 percent glucose. So there’s really not much of a difference between the two.”
Chapter 7 – The Ticker
Mechanics of Heart Disease
- “Globally, heart disease and stroke (or cerebrovascular disease), which I lump together under the single heading of atherosclerotic cardiovascular disease, or ASCVD, represent the leading cause of death, killing an estimated 2,300 people every day in the United States, according to the CDC—more than any other cause, including cancer.”
- “While heart disease is the most prevalent age-related condition, it is also more easily prevented than either cancer or Alzheimer’s disease.”
- “I’ll never forget the one-question pop quiz that Allan Sniderman dropped on me over dinner at Dulles Airport, back in 2014: “What proportion of heart attacks occur in people younger than age sixty-five?” I guessed high, one in four, but I was way low. Fully half of all major adverse cardiovascular events in men (and a third of those in women), such as heart attack, stroke, or any procedure involving a stent or a graft, occur before the age of sixty-five. In men, one-quarter of all events occur before age fifty-four.”
- “It is not an accident that the two biggest risk factors for heart disease, smoking and high blood pressure, cause damage to the endothelium. Smoking damages it chemically, while high blood pressure does so mechanically, but the end result is endothelial harm that, in turn, leads to greater retention of LDL.”
- “If the plaque does become unstable, eroding or even rupturing, you’ve really got problems. The damaged plaque may ultimately cause the formation of a clot, which can narrow and ultimately block the lumen of the blood vessel—or worse, break free and cause a heart attack or stroke. This is why we worry more about the noncalcified plaques than the calcified ones. Normally, however, most atherosclerotic plaques are fairly undramatic.”
Cholesterol
- “The reason they’re called high- and low-density lipoproteins (HDL and LDL, respectively) has to do with the amount of fat relative to protein that each one carries. LDLs carry more lipids, while HDLs carry more protein in relation to fat, and are therefore more dense.”
- “Eating lots of saturated fat can increase levels of atherosclerosis-causing lipoproteins in blood, but most of the actual cholesterol that we consume in our food ends up being excreted out our backsides. The vast majority of the cholesterol in our circulation is actually produced by our own cells.”
- ““There’s no connection whatsoever between cholesterol in food and cholesterol in blood,” Keys said in a 1997 interview. “None. And we’ve known that all along. Cholesterol in the diet doesn’t matter at all unless you happen to be a chicken or a rabbit.” It took nearly two more decades before the advisory committee responsible for the US government dietary guidelines finally conceded (in 2015) that “cholesterol is not a nutrient of concern for overconsumption.” Glad we settled that.”
- “Newer research suggests that HDL has multiple other atheroprotective functions that include helping maintain the integrity of the endothelium, lowering inflammation, and neutralizing or stopping the oxidation of LDL, like a kind of arterial antioxidant.”
- “The cholesterol content in your LDL particles, your “bad” cholesterol number (technically expressed as LDL-C),[*3] is actually a decent if imperfect proxy for its biologic impact; lots of studies have shown a strong correlation between LDL-C and event risk. But the all-important “good cholesterol” number on your blood test, your HDL-C, doesn’t actually tell me very much if anything about your overall risk profile. Risk does seem to decline as HDL-C rises to around the 80th percentile. But simply raising HDL cholesterol concentrations by brute force, with specialized drugs, has not been shown to reduce cardiovascular risk at all.”
- “Atherosclerosis probably would not occur [emphasis mine] in the absence of LDL-C concentrations in excess of physiological needs (on the order of 10 to 20 mg/dL).””
- “And lo and behold, it turns out that low LDL cholesterol does not cause cancer or increase its risk. If we use the same technique to look at the effect of LDL levels on cardiovascular disease (our dependent variable), it turns out that higher LDL cholesterol is causally linked to the development of cardiovascular disease (as we’ll discuss in chapter 7).”
apoB
- “I’ve been saying LDL, but the key factor here is actually exposure to apoB-tagged particles, over time.”
- “So to gauge the true extent of your risk, we have to know how many of these apoB particles are circulating in your bloodstream. That number is much more relevant than the total quantity of cholesterol that these particles are carrying.”
- “evidence has piled up pointing to apoB as far more predictive of cardiovascular disease than simply LDL-C, the standard “bad cholesterol” measure. According to an analysis published in JAMA Cardiology in 2021, each standard-deviation increase in apoB raises the risk of myocardial infarction by 38 percent in patients without a history of cardiac events or a diagnosis of cardiovascular disease (i.e., primary prevention). That’s a powerful correlation.”
- “I have all my patients tested for apoB regularly, and you should ask for the same test the next time you see your doctor. (Don’t be waved off by nonsensical arguments about “cost”: It’s about twenty to thirty dollars.)”
- “As we’ll discuss in the final section, I take a very hard line on lowering apoB, the particle that causes all this trouble. (In short: get it as low as possible, as early as possible.)”
- “In my clinical experience, about a third to half of people who consume high amounts of saturated fats (which sometimes goes hand in hand with a ketogenic diet) will experience a dramatic increase in apoB particles, which we obviously don’t want.[*8] Monounsaturated fats, found in high quantities in extra virgin olive oil, macadamia nuts, and avocados (among other foods), do not have this effect, so I tend to push my patients to consume more of these, up to about 60 percent of total fat intake. The point is not necessarily to limit fat overall but to shift to fats that promote a better lipid profile.”
Lp(a)
- “But because Lp(a) is a member of the apoB particle family, it also has the potential to penetrate the endothelium and get lodged in an artery wall; because of its structure, Lp(a) may be even more likely than a normal LDL particle to get stuck, with its extra cargo of lipids gone bad. Even worse, once in there, it acts partly as a thrombotic or proclotting factor, which helps to speed the formation of arterial plaques.”
- “This is why, if you have a history of premature heart attacks in your family, you should definitely ask for an Lp(a) test. We test every single patient for Lp(a) during their first blood draw. Because elevated Lp(a) is largely genetic, the test need only be done once (and cardiovascular disease guidelines are beginning to advise a once-a-lifetime test for it anyway).”
- “There was no quick fix for Anahad, or anyone else with elevated Lp(a). It does not seem to respond to behavioral interventions such as exercise and dietary changes the way that, say, LDL-C does. A class of drug called PCSK9 inhibitors, aimed at lowering apoB concentrations, does seem to be able to reduce Lp(a) levels by approximately 30 percent, but as yet there are no data suggesting that they reduce the excess events (heart attacks) attributable to that particle. Thus, the only real treatment for elevated Lp(a) right now is aggressive management of apoB overall.”
- “Simply put, I think you can’t lower apoB and LDL-C too much, provided there are no side effects from treatment. You want it as low as possible.”
- “Once you understand that apoB particles—LDL, VLDL, Lp(a)—are causally linked to ASCVD, the game completely changes. The only way to stop the disease is to remove the cause, and the best time to do that is now.”
Statins
- “But for many patients, if not for most, lowering apoB to the levels we aim for—the physiologic levels found in children—cannot be accomplished with diet alone, so we need to use nutritional interventions in tandem with drugs.”
- “Statins are far and away the most prescribed class of drugs for lipid management, but there are several other options that might be right for a given individual, and often we need to combine classes of drugs, so it’s not uncommon for a patient to take two lipid-lowering drugs that operate via distinct mechanisms.”
- “These are typically thought of as “cholesterol-lowering” medications, but I think we are better served to think about them in terms of increasing apoB clearance, enhancing the body’s ability to get apoBs out of circulation.”
- “For every seven people who are put on a statin at this early stage, we could potentially save one life. The reason for this is simple math: risk is proportional to apoB exposure over time.”
- “While there are seven statins on the market, I tend to start with rosuvastatin (Crestor) and only pivot from that if there is some negative effect from the drug (e.g., a symptom or biomarker).”
- “For people who can’t tolerate statins, I like to use a newer drug, called bempedoic acid (Nexletol), which manipulates a different pathway to accomplish much the same end..”
- “Ethyl eicosapentaenoic acid (Vascepa), a drug derived from fish oil and consisting of four grams of pharmaceutical-grade eicosapentaenoic acid (EPA), also has FDA approval to reduce LDL in patients with elevated triglycerides.”
Time Horizon
- “Atherosclerosis is with us, in some form, throughout our life course. Yet most doctors consider it “overtreatment” to intervene if a patient’s computed ten-year risk of a major adverse cardiac event (e.g., heart attack or stroke) is below 5 percent, arguing that the benefits are not greater than the risks, or that treatment costs too much. In my opinion, this betrays a broader ignorance about the inexorable, long-term unfolding of heart disease. Ten years is far too short a time horizon. If we want to reduce deaths from cardiovascular disease, we need to begin thinking about prevention in people in their forties and even thirties.”
- “Another way to think of all this is that someone might be considered “low risk” at a given point—but on what time horizon? The standard is ten years. But what if our time horizon is “the rest of your life”?”
- “Yet most physicians and cardiology experts would still insist that one’s thirties are too young to begin to focus on primary prevention of cardiac disease. This viewpoint is directly challenged by a 2018 JAMA Cardiology paper coauthored by Allan Sniderman, comparing ten-year versus thirty-year risk horizons in terms of prevention. Sniderman and colleagues’ analysis found that looking at a thirty-year time frame rather than the standard ten years and taking aggressive precautionary measures early—like beginning statin treatment earlier in certain patients—could prevent hundreds of thousands more cardiac events, and by implication could save many lives.”
- “We know that smoking is causally linked to lung cancer. Should we tell someone to stop smoking only after their ten-year risk of lung cancer reaches a certain threshold?”
Chapter 8 – The Runaway Cell
If the first rule of cancer is “Don’t get cancer,” the second rule is “Catch it as soon as possible.”
Peter Attia – Outlive
What is Cancer?
- “Contrary to popular belief, cancer cells don’t grow faster than their noncancerous counterparts; they just don’t stop growing when they are supposed to.”
- “The second property that defines cancer cells is their ability to travel from one part of the body to a distant site where they should not be. This is called metastasis…”
- “One of the biggest obstacles to a “cure” is the fact that cancer is not one single, simple, straightforward disease, but a condition with mind-boggling complexity.”
- “In fact, there didn’t seem to be any individual genes that “caused” cancer at all; instead, it seemed to be random somatic mutations that combined to cause cancers.”
- “Breast cancer kills only when it becomes metastatic. Prostate cancer kills only when it becomes metastatic. You could live without either of those organs.”
- “Five decades into the war on cancer, it seems clear that no single “cure” is likely to be forthcoming. Rather, our best hope likely lies in figuring out better ways to attack cancer on all three of these fronts: prevention, more targeted and effective treatments, and comprehensive and accurate early detection.”
Prevention
Of all the Horsemen, cancer is probably the hardest to prevent. It is probably also the one where bad luck in various forms plays the greatest role, such as in the form of accumulated somatic mutations. The only modifiable risks that really stand out in the data are smoking, insulin resistance, and obesity (all to be avoided)—and maybe pollution (air, water, etc.), but the data here are less clear.
Peter Attia – Outlive
- “And extreme obesity (BMI ≥ 40) is associated with a 52 percent greater risk of death from all cancers in men, and 62 percent in women.”
- “I suspect that the association between obesity, diabetes, and cancer is primarily driven by inflammation and growth factors such as insulin.”
- “Thus, insulin acts as a kind of cancer enabler, accelerating its growth. Source: NCI (2022a). This in turn suggests that metabolic therapies, including dietary manipulations that lower insulin levels, could potentially help slow the growth of some cancers and reduce cancer risk.”
- “I’m not suggesting that it’s possible to “starve” cancer or that any particular diet will magically make cancer go away; cancer cells always seem to be able to obtain the energy supply they need. What I am saying is that we don’t want to be anywhere on that spectrum of insulin resistance to type 2 diabetes, where our cancer risk is clearly elevated. To me, this is the low-hanging fruit of cancer prevention, right up there with quitting smoking.“
I would go so far as to argue that early detection is our best hope for radically reducing cancer mortality.
Peter Attia – Outlive
Detection
- “Out of dozens of different types of cancers, we have agreed-upon, reliable screening methods for only five: lung (for smokers), breast, prostate, colorectal, and cervical. Even so, mainstream guidelines have been waving people away from some types of early screening, such as mammography in women and blood testing for PSA, prostate-specific antigen, in men. In part this has to do with cost, and in part this has to do with the risk of false positives that may lead to unnecessary or even dangerous treatment (entailing further costs).”
Liquid Biopsies
- “I am also cautiously optimistic about pairing these tried-and-true staples of cancer screening with emerging methods, such as “liquid biopsies,” which can detect trace amounts of cancer-cell DNA via a simple blood test.”
- “Using very-high-throughput screening and a massive AI engine, the Galleri test can glean two crucial pieces of information from this sample of blood: Is cancer present? And if so, where is it? From what part of the body did it most likely originate?”
- “In this study, the Galleri test proved to have a very high specificity, about 99.5 percent, meaning only 0.5 percent of tests yielded a false positive. If the test says you have cancer, somewhere in your body, then it is likely that you do. The trade-off is that the resulting sensitivity can be low, depending on the stage. (That is, even if the test says you don’t have cancer, you are not necessarily in the clear.)”
Think asymmetric risk: It’s possible that not screening early and frequently enough is the most dangerous option.
Peter Attia – Outlive
False Positives
- “In fact, in this low-risk group, the “positive predictive value” of mammography is only about 10 percent—meaning that if you do test positive, there is only about a one-in-ten chance that you actually have breast cancer. In other populations, with greater overall prevalence (and risk), the test performs much better.”
- “We need to think in terms of stacking test modalities—incorporating ultrasound and MRI in addition to mammography, for example, when looking for breast cancer. With multiple tests, our resolution improves and fewer unnecessary procedures will be performed.”
- “Despite all this, even something as advanced as the best DWI MRI is not without problems, if used in isolation. While the sensitivity of this test is very high (meaning it’s very good at finding cancer if cancer is there, hence very few false negatives), the specificity is relatively low (which means it’s not as good at telling you when you don’t have cancer, hence a lot of false positives). … The more you increase one, the more you decrease the other.”
The key question we want to answer is, Will our patient die with prostate cancer, as many men do, or will he die from it?
Peter Attia – Outlive
Colonoscopy
- “The purpose of the colonoscopy is to look not only for full-fledged tumors but also for polyps, which are growths that form in the lining of the colon. … Not all polyps become cancer, but all colon cancers came from polyps.”
- “In my practice, we go further, typically encouraging average-risk individuals to get a colonoscopy by age forty—and even sooner if anything in their history suggests they may be at higher risk.”
- “Two or three years might seem like a very short window of time to repeat such an involved procedure, but colon cancer has been documented to appear within the span of as little as six months to two years after a normal colonoscopy.”
Warbug Effect
- “In the 1920s, a German physiologist named Otto Warburg discovered that cancer cells had a strangely gluttonous appetite for glucose, devouring it at up to forty times the rate of healthy tissues.”
- “This phenomenon was dubbed the Warburg effect, and even today, one way to locate potential tumors is by injecting the patient with radioactively labeled glucose and then doing a PET scan to see where most of the glucose is migrating. Areas with abnormally high glucose concentrations indicate the possible presence of a tumor.”
- “The Warburg effect, also known as anaerobic glycolysis, turns the same amount of glucose into a little bit of energy and a whole lot of chemical building blocks—which are then used to build new cells rapidly. Thus, the Warburg effect is how cancer cells fuel their own proliferation. But it also represents a potential vulnerability in cancer’s armor.”
Treatment
- “Combining surgery and radiation therapy is pretty effective against most local, solid-tumor cancers. But while we’ve gotten fairly good at this approach, we have essentially maxed out our ability to treat cancers this way.”
- “And surgery is of limited value when cancer has metastasized, or spread. Metastatic cancers can be slowed by chemotherapy, but they virtually always come back, often more resistant to treatment than ever.”
- “Meanwhile, as cancer researcher Robert Gatenby points out, those cancer cells that do manage to survive chemotherapy often end up acquiring mutations that make them stronger, like cockroaches that develop resistance to insecticides.”
- “Contrary to popular belief, killing cancer cells is actually pretty easy.”
- “The game is won by killing cancers while sparing the normal cells. Selective killing is the key.”
- “Ultimately, successful treatments will need to be both systemic and specific to a particular cancer type.”
Immunotherapy
- “I feel that immunotherapy, in particular, has enormous promise.”
- “As of yet, the various immunotherapy treatments that have been approved still benefit only a fairly small percentage of patients. About a third of cancers can be treated with immunotherapy, and of those patients, just one-quarter will actually benefit (i.e., survive). That means that only 8 percent of potential cancer deaths could be prevented by immunotherapy, according to an analysis by oncologists Nathan Gay and Vinay Prasad.”
- “But when patients do respond to immunotherapy, and go into complete remission, they often stay in remission. Between 80 and 90 percent of so-called complete responders to immunotherapy remain disease-free fifteen years out.”
- “It took many more years and several iterations, but Rosenberg and his team adapted a technique that had been developed in Israel that involved taking T cells from a patient’s blood, then using genetic engineering to add antigen receptors that were specifically targeted to the patient’s tumors. Now the T cells were programmed to attack the patient’s cancer. Known as chimeric antigen receptor T cells (or CAR-T), these modified T cells could be multiplied in the lab and then infused back into the patient.”
- “Instead of activating T cells to go kill the cancer, the checkpoint inhibitors help make the cancer visible to the immune system.”
- “One very promising technique is called adoptive cell therapy (or adoptive cell transfer, ACT). ACT is a class of immunotherapy whereby supplemental T cells are transferred into a patient, like adding reinforcements to an army, to bolster their ability to fight their own tumor. These T cells have been genetically programmed with antigens specifically targeted at the patient’s individual tumor type.”
- “ACT effectively means designing a new, customized anticancer drug for each individual patient. This is obviously a costly proposition, and a very labor-intensive process, but it has a lot of promise. The proof of principle is here, but much more work is needed, not only to improve the efficacy of this approach but also to enable us to deliver this treatment more widely and more easily.”
Dietary Intervention
- “The results are important because they show not only that a cancer cell’s metabolism is a valid target for therapy but that a patient’s metabolic state can affect the efficacy of a drug. In this case, the animals’ ketogenic diet seemed to synergize with what was otherwise a somewhat disappointing treatment, and together they proved to be far more powerful than either one alone.”
- “Work by Valter Longo of the University of Southern California and others has found that fasting, or a fasting-like diet, increases the ability of normal cells to resist chemotherapy, while rendering cancer cells more vulnerable to the treatment.””A randomized trial in 131 cancer patients undergoing chemotherapy found that those who were placed on a “fasting-mimicking diet” (basically, a very low-calorie diet designed to provide essential nutrients while reducing feelings of hunger) were more likely to respond to chemotherapy and to feel better physically and emotionally.”
- “As Keith Flaherty, a medical oncologist and the director of developmental therapeutics at Massachusetts General Hospital, explained to me, the best strategy to target cancer is likely by targeting multiple vulnerabilities of the disease at one time, or in sequence. By stacking different therapies, such as combining a PI3K inhibitor with a ketogenic diet, we can attack cancer on multiple fronts, while also minimizing the likelihood of the cancer developing resistance (via mutations) to any single treatment.”
Chapter 9 – Chasing Memory
Broadly, our strategy should be based on the following principles: WHAT’S GOOD FOR THE HEART IS GOOD FOR THE BRAIN. That is, vascular health (meaning low apoB, low inflammation, and low oxidative stress) is crucial to brain health. WHAT’S GOOD FOR THE LIVER (AND PANCREAS) IS GOOD FOR THE BRAIN. Metabolic health is crucial to brain health. TIME IS KEY. We need to think about prevention early, and the more the deck is stacked against you genetically, the harder you need to work and the sooner you need to start. As with cardiovascular disease, we need to play a very long game. OUR MOST POWERFUL TOOL FOR PREVENTING COGNITIVE DECLINE IS EXERCISE. We’ve talked a lot about diet and metabolism, but exercise appears to act in multiple ways (vascular, metabolic) to preserve brain health; we’ll get into more detail in Part III, but exercise—lots of it—is a foundation of our Alzheimer’s-prevention program.
Peter Attia – Outlive
Alzheimer’s Disease
- “Alzheimer’s disease is perhaps the most difficult, most intractable of the Horsemen diseases.”
- “It appears, then, that the presence of amyloid-beta plaques may be neither necessary for the development of Alzheimer’s disease nor sufficient to cause it.”
- “While female Alzheimer’s patients outnumber men by two to one, the reverse holds true for Lewy body dementia and Parkinson’s, both of which are twice as prevalent in men.”
Risk Factors
- “One important section of the cognitive testing evaluates the patient’s sense of smell. Can they correctly identify scents such as coffee, for example? Olfactory neurons are among the first to be affected by Alzheimer’s disease.”
- “Having type 2 diabetes doubles or triples your risk of developing Alzheimer’s disease, about the same as having one copy of the APOE e4 gene.”
- “Insulin seems to play a key role in memory function. Insulin receptors are highly concentrated in the hippocampus, the memory center of the brain. Several studies have found that spraying insulin right into subjects’ noses—administering it as directly as possible into their brains—quickly improves cognitive performance and memory, even in people who have already been diagnosed with Alzheimer’s disease.”
- “Another somewhat surprising risk factor that has emerged is hearing loss. Studies have found that hearing loss is clearly associated with Alzheimer’s disease, but it’s not a direct symptom. Rather, it seems hearing loss may be causally linked to cognitive decline, because folks with hearing loss tend to pull back and withdraw from interactions with others. When the brain is deprived of inputs—in this case auditory inputs—it withers.”
Prevention & Treatment
- “Sleep is also a very powerful tool against Alzheimer’s disease, as we’ll see in chapter 16.”
- “Another surprising intervention that may help reduce systemic inflammation, and possibly Alzheimer’s disease risk, is brushing and flossing one’s teeth.”
- “The best interpretation I can draw from the literature suggests that at least four sessions per week, of at least twenty minutes per session, at 179 degrees Fahrenheit (82 degrees Celsius) or hotter seems to be the sweet spot to reduce the risk of Alzheimer’s by about 65 percent (and the risk of ASCVD by 50 percent).”
Exercise Intervention
- “The single most powerful item in our preventive tool kit is exercise, which has a two-pronged impact on Alzheimer’s disease risk: it helps maintain glucose homeostasis, and it improves the health of our vasculature.”
- “Evidence also demonstrates a linear relationship between cognitive decline and increased intimal media thickness in the carotid artery, a major blood vessel that feeds the brain.”
- “The more of these networks and subnetworks that we have built up over our lifetime, via education or experience, or by developing complex skills such as speaking a foreign language or playing a musical instrument, the more resistant to cognitive decline we will tend to be. The brain can continue functioning more or less normally, even as some of these networks begin to fail. This is called “cognitive reserve,” and it has been shown to help some patients to resist the symptoms of Alzheimer’s disease.”
- “There is a parallel concept known as “movement reserve” that becomes relevant with Parkinson’s disease. People with better movement patterns, and a longer history of moving their bodies, such as trained or frequent athletes, tend to resist or slow the progression of the disease as compared to sedentary people.”
- “Exercise is the only intervention shown to delay the progression of Parkinson’s.”
- “The evidence suggests that tasks or activities that present more varied challenges, requiring more nimble thinking and processing, are more productive at building and maintaining cognitive reserve. Simply doing a crossword puzzle every day, on the other hand, seems only to make people better at doing crossword puzzles. The same goes for movement reserve: dancing appears to be more effective than walking at delaying symptoms of Parkinson’s disease, possibly because it involves more complex movement.”
- “Strength training is likely just as important. A study looking at nearly half a million patients in the United Kingdom found that grip strength, an excellent proxy for overall strength, was strongly and inversely associated with the incidence of dementia (see figure 8).”

Dietary Intervention
- “Because metabolism plays such an outsize role with at-risk e4 patients like Stephanie, our first step is to address any metabolic issues they may have. Our goal is to improve glucose metabolism, inflammation, and oxidative stress. One possible recommendation for someone like her would be to switch to a Mediterranean-style diet, relying on more monounsaturated fats and fewer refined carbohydrates, in addition to regular consumption of fatty fish.”
- “Studies in Alzheimer’s patients find that while their brains become less able to utilize glucose, their ability to metabolize ketones does not decline.”
- “A systematic review of randomized controlled trials found that ketogenic therapies improved general cognition and memory in subjects with mild cognitive impairment and early-stage Alzheimer’s disease.”
Part III
Chapter 10 – Thinking Tactically
“In Medicine 3.0, we have five tactical domains that we can address in order to alter someone’s health.
- The first is exercise, which I consider to be by far the most potent domain in terms of its impact on both lifespan and healthspan.
- Next is diet or nutrition—or as I prefer to call it, nutritional biochemistry.
- The third domain is sleep, which has gone underappreciated by Medicine 2.0 until relatively recently.
- The fourth domain encompasses a set of tools and techniques to manage and improve emotional health.
- Our fifth and final domain consists of the various drugs, supplements, and hormones that doctors learn about in medical school and beyond. I lump these into one bucket called exogenous molecules, meaning molecules we ingest that come from outside the body.”
When I evaluate new patients, I’m always asking three key questions:
- Are they overnourished or undernourished? That is, are they taking in too many or too few calories?
- Are they undermuscled or adequately muscled?
- Are they metabolically healthy or not?
Chapter 11 – Exercise
So if you adopt only one new set of habits based on reading this book, it must be in the realm of exercise.
Peter Attia – Outlive
Benefits
- “The data demonstrating the effectiveness of exercise on lifespan are as close to irrefutable as one can find in all human biology. Yet if anything, I think exercise is even more effective at preserving healthspan than extending lifespan. There is less hard evidence here, but I believe that this is where exercise really works its magic when applied correctly. I tell my patients that even if exercise shortened your life by a year (which it clearly does not), it would still be worthwhile purely for the healthspan benefits, especially in middle age and beyond.”
- “But at least five factors[*3] increase my confidence in at least the partial causality of this relationship. First, the magnitude of the effect size is very large. Second, the data are consistent and reproducible across many studies of disparate populations. Third, there is a dose-dependent response (the fitter you are, the longer you live). Fourth, there is great biologic plausibility to this effect, via the known mechanisms of action of exercise on lifespan and healthspan. And fifth, virtually all experimental data on exercise in humans suggest that it supports improved health.”
- “Exercise is by far the most potent longevity “drug.” No other intervention does nearly as much to prolong our lifespan and preserve our cognitive and physical function. But most people don’t do nearly enough—and exercising the wrong way can do as much harm as good.”
- “I used to prioritize nutrition over everything else, but I now consider exercise to be the most potent longevity “drug” in our arsenal, in terms of lifespan and healthspan. The data are unambiguous: exercise not only delays actual death but also prevents both cognitive and physical decline, better than any other intervention.”
- “There are reams of data supporting the notion that even a fairly minimal amount of exercise can lengthen your life by several years.”
- “Going from zero weekly exercise to just ninety minutes per week can reduce your risk of dying from all causes by 14 percent.”
VO2 Max
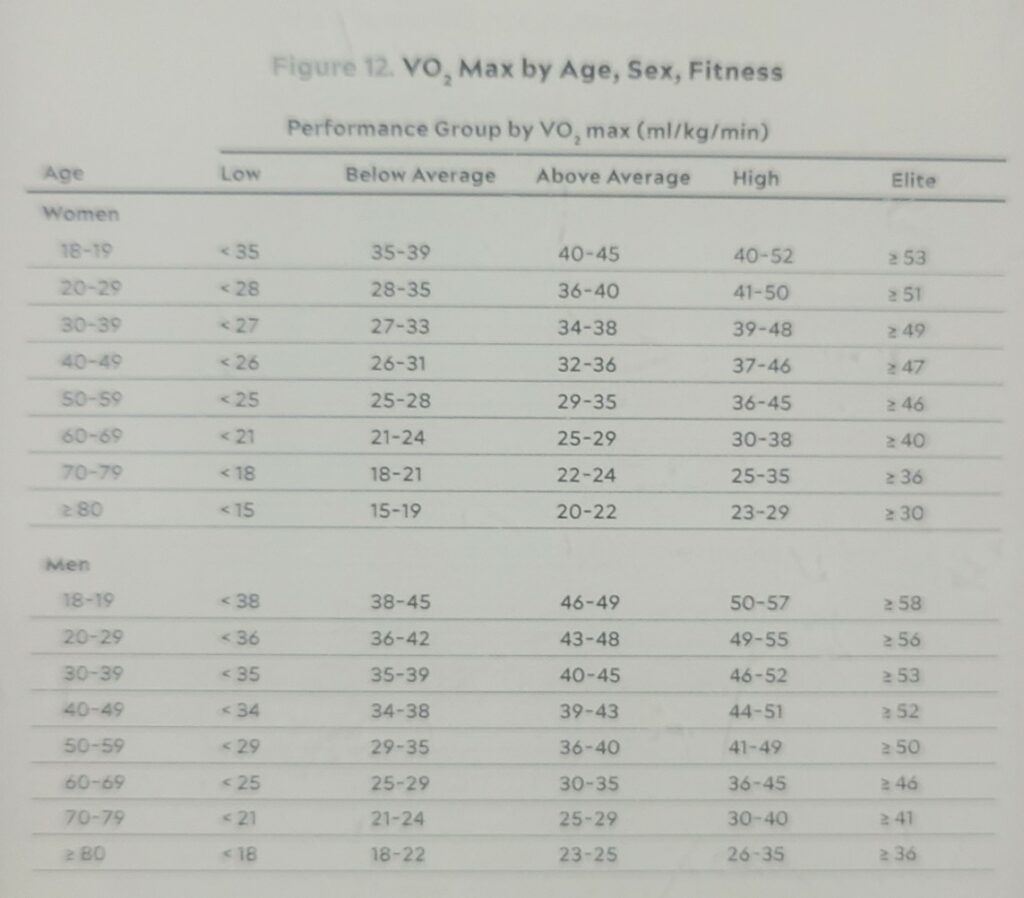
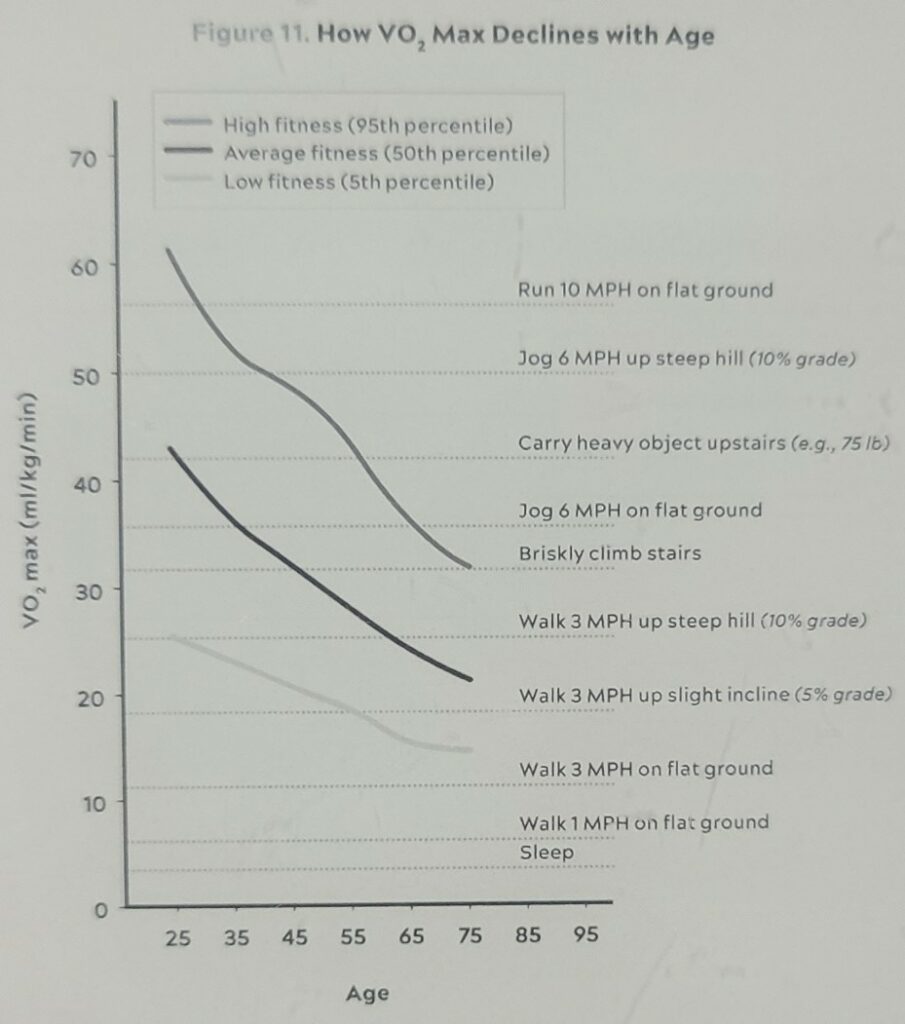
- “It turns out that peak aerobic cardiorespiratory fitness, measured in terms of VO2 max, is perhaps the single most powerful marker for longevity. VO2 max represents the maximum rate at which a person can utilize oxygen. This is measured, naturally, while a person is exercising at essentially their upper limit of effort.”
- “VO2 max is typically expressed in terms of the volume of oxygen a person can use, per kilogram of body weight, per minute. An average forty-five-year-old man will have a VO2 max around 40 ml/kg/min, while an elite endurance athlete will likely score in the high 60s and above. An unfit person in their thirties or forties, on the other hand, might score only in the high 20s on a VO2 max test, according to Mike Joyner, an exercise physiologist and researcher at the Mayo Clinic.”
- “A person who smokes has a 40 percent greater risk of all-cause mortality (that is, risk of dying at any moment) than someone who does not smoke, representing a hazard ratio or (HR) of 1.40. This study found that someone of below-average VO2 max for their age and sex (that is, between the 25th and 50th percentiles) is at double the risk of all-cause mortality compared to someone in the top quartile (75th to 97.6th percentiles). Thus, poor cardiorespiratory fitness carries a greater relative risk of death than smoking.“
Muscle Mass & Strength
- “A ten-year observational study of roughly 4,500 subjects ages fifty and older found that those with low muscle mass were at 40 to 50 percent greater risk of mortality than controls, over the study period. Further analysis revealed that it’s not the mere muscle mass that matters but the strength of those muscles, their ability to generate force.”
- “As figure 10 reveals, falls are by far the leading cause of accidental deaths in those ages sixty-five and older—and this is without even counting the people who die three or six or twelve months after their nonfatal but still serious fall pushed them into a long and painful decline.”
Centenarian Decathlon
Think of the Centenarian Decathlon as the ten most important physical tasks you will want to be able to do for the rest of your life.
- Hike 1.5 miles on a hilly trail.
- Get up off the floor under your own power, using a maximum of one arm for support.
- Pick up a young child from the floor.
- Carry two five-pound bags of groceries for five blocks.
- Lift a twenty-pound suitcase into the overhead compartment of a plane.
- Balance on one leg for thirty seconds, eyes open. (Bonus points: eyes closed, fifteen seconds.)
- Have sex.
- Climb four flights of stairs in three minutes.
- Open a jar.
- Do thirty consecutive jump-rope skips.
- “The record for the hundred-meter dash for women ages one hundred and up is about forty-one seconds.” LOL
- “Over the next thirty or forty years, your muscle strength will decline by about 8 to 17 percent per decade—accelerating as time goes on. So if you want to pick up that thirty-pound grandkid or great-grandkid when you’re eighty, you’re going to have to be able to lift about fifty to fifty-five pounds now. Without hurting yourself. Can you do that?”
- Determine your current decathlon challenge to be on pace for your centenarian decathlon (APP).
- “Together, we come up with a list of ten or fifteen events in their personal Centenarian Decathlon, representing their goals for their later decades. This then determines how they should be training.”
- “The beauty of the Centenarian Decathlon is that it is broad yet unique to each individual. Nor is it limited to ten events; for most people it ends up being more, depending on their goals.”
- “When my patients say they are more interested in being kick-ass fifty-year-olds than Centenarian Decathletes, I reply that there is no better way to make that happen than to set a trajectory toward being vibrant at one hundred (or ninety, or eighty) just as an archer who trains at 100 yards will be more accurate at 50.”
- “As Centenarian Decathletes, we are no longer training for a specific event, but to become a different sort of athlete altogether: an athlete of life.”
Chapter 12 – Training 101
The three dimensions in which we want to optimize our fitness are aerobic endurance and efficiency (aka cardio), strength, and stability.
PETER ATTIA – OUTLIVE
Aerobic Endurance & Efficiency (Cardio)
- “The various levels of intensity all count as cardio but are fueled by multiple different energy systems. For our purposes, we are interested in two particular regions of this continuum: long, steady endurance work, such as jogging or cycling or swimming, where we are training in what physiologists call zone 2, and maximal aerobic efforts, where VO2 max comes into play.”
Zone 2
- “Zone 2 is more or less the same in all training models: going at a speed slow enough that one can still maintain a conversation but fast enough that the conversation might be a little strained.”
- “If you know your maximum heart rate—not estimated, but your actual maximum, the highest number you’ve ever seen on a heart rate monitor—your zone 2 will correspond to between approximately 70 and 85 percent of that peak number, depending on your fitness levels. That’s a big range, so when starting people out, I prefer they rely on their rate of perceived exertion, or RPE, also known as the “talk test.””
- “Typically, someone working at a lower relative intensity will be burning more fat, while at higher intensities they would rely more on glucose. The healthier and more efficient your mitochondria, the greater your ability to utilize fat, which is by far the body’s most efficient and abundant fuel source. This ability to use both fuels, fat and glucose, is called “metabolic flexibility,” and it is what we want.”
- “They had each group ride a stationary bicycle at a given level of intensity relative to their fitness (about 80 percent of their maximum heart rate), while the scientists analyzed the amount of oxygen they consumed and the CO2 they exhaled in order to determine how efficiently they produced power—and what primary fuels they were using. The differences they found were striking. The professional cyclists could zoom along, producing a huge amount of power while still burning primarily fat. But the subjects with metabolic syndrome relied almost entirely on glucose for their fuel source, even from the first pedal stroke. They had virtually zero ability to tap into their fat stores, meaning they were metabolically inflexible: able to use only glucose but not fat.”
- “A professional cyclist might spend thirty to thirty-five hours a week training on his or her bike, and 80 percent of that time in zone 2.”
- “(The catch is that a professional rider’s zone 2 output feels like zone 5 for most people.)”
- “In technical terms, San Millán describes zone 2 as the maximum level of effort that we can maintain without accumulating lactate.”
- “Because I am a numbers guy and I love biomarkers and feedback, I often test my own lactate while I am working out this way, using a small handheld lactate monitor, to make sure my pacing is correct. The goal is to keep lactate levels constant, ideally between 1.7 and 2.0 millimoles.”
- “Mitochondria are incredibly plastic, and when we do aerobic exercise, it stimulates the creation of many new and more efficient mitochondria through a process called mitochondrial biogenesis, while eliminating ones that have become dysfunctional via a recycling process called mitophagy (which is like autophagy, touched on in chapter 5, but for mitochondria). A person who exercises frequently in zone 2 is improving their mitochondria with every run, swim, or bike ride. But if you don’t use them, you lose them.”
- “Chronic blood glucose elevations damage organs from our heart to our brain to our kidneys and nearly everything in between—even contributing to erectile dysfunction in men.”
- “This in turn explains why exercise, especially in zone 2, can be so effective in managing both type 1 and type 2 diabetes: It enables the body to essentially bypass insulin resistance in the muscles to draw down blood glucose levels. I have one patient with type 1 diabetes, meaning he produces zero insulin, who keeps his glucose in check almost entirely by walking briskly for six to ten miles every day, and sometimes more.”
- “The key is to find an activity that fits into your lifestyle, that you enjoy doing, and that enables you to work at a steady pace that meets the zone 2 test: You’re able to talk in full sentences, but just barely.”
- “Based on multiple discussions with San Millán and other exercise physiologists, it seems that about three hours per week of zone 2, or four 45-minute sessions, is the minimum required for most people to derive a benefit and make improvements, once you get over the initial hump of trying it for the first time.”
- “One way to track your progression in zone 2 is to measure your output in watts at this level of intensity. … You take your average wattage output for a zone 2 session and divide it by your weight to get your watts per kilogram, which is the number we care about. So if you weigh 60 kilos (about 132 pounds) and can generate 125 watts in zone 2, that works out to a bit more than 2 watts/kg, which is about what one would expect from a reasonably fit person.”
- “Zone 2 can be a bit boring on its own, so I typically use the time to listen to podcasts or audiobooks, or just think about issues that I’m working on”
VO2 Max
- “Typically, for patients who are new to exercising, we introduce VO2 max training after about five or six months of steady zone 2 work.”
- “Testing is widely available, even from some of the larger fitness chains. The bad news is that the VO2 max test is an unpleasant affair that entails riding an exercise bike or running on a treadmill at ever greater intensity, while wearing a mask designed to measure oxygen consumption and CO2 production. The peak amount of oxygen you consume, typically close to the point at which you “fail,” meaning the point where you just can’t keep going, yields your VO2 max. We have all our patients do the test at least annually, and they almost all hate it. We then compare their results, normalized by weight, to the population of their age and sex.”
- “Ideally, I want them to target the “elite” range for their age and sex (roughly the top 2 percent). If they achieve that level, I say good job—now let’s reach for the elite level for your sex, but two decades younger.”
- “Studies suggest that your VO2 max will decline by roughly 10 percent per decade—and up to 15 percent per decade after the age of fifty.”
- “Improving your VO2 max from the very bottom quartile to the quartile above (i.e., below average) is associated with almost a 50 percent reduction in all-cause mortality, as we saw earlier.”
- “One study found that boosting elderly subjects’ VO2 max by 6 ml/kg/min, or about 25 percent, was equivalent to subtracting twelve years from their age.”
- “The beauty of this is that VO2 max can always be improved by training, no matter how old you are. Don’t believe me? Then let me introduce you to an amazing Frenchman named Robert Marchand, who set an age-group world record in 2012 by cycling 24.25 kilometers in an hour, at the age of 101. Apparently, he wasn’t satisfied with that performance, so he decided he needed to train harder. Following a strict program designed by top coaches and physiologists, he managed to boost his VO2 max from an already-impressive 31 ml/kg/min up to 35 ml/kg/min, which would put him in the elite 2.5 percent of men in their eighties. Two years later, now 103, he came back and broke his own record, riding almost twenty-seven kilometers in an hour.”
- “Where HIIT intervals are very short, typically measured in seconds, VO2 max intervals are a bit longer, ranging from three to eight minutes—and a notch less intense.”
- “The tried-and-true formula for these intervals is to go four minutes at the maximum pace you can sustain for this amount of time—not an all-out sprint, but still a very hard effort. Then ride or jog four minutes easy, which should be enough time for your heart rate to come back down to below about one hundred beats per minute. Repeat this four to six times and cool down.”
- “A single workout per week in this zone will generally suffice. You’ll pretty quickly find that it boosts your performance across the rest of your exercise program as well—and, more importantly, in the rest of your life.”
Strength
I think of strength training as a form of retirement saving. Just as we want to retire with enough money saved up to sustain us for the rest of our lives, we want to reach older age with enough of a “reserve” of muscle (and bone density) to protect us from injury and allow us to continue to pursue the activities that we enjoy.
PETER ATTIA – OUTLIVE
- “But muscle mass may be the least important metric here. According to Andy Galpin, a professor of kinesiology at California State University, Fullerton, and one of the foremost authorities on strength and performance, we lose muscle strength about two to three times more quickly than we lose muscle mass. And we lose power (strength x speed) two to three times faster than we lose strength.”
- Sarcopenia is a prime marker for a broader clinical condition called frailty, where a person meets three of these five criteria:
- unintended weight loss
- exhaustion or low energy
- low physical activity
- slowness in walking
- weak grip strength (about which more soon).
- “One study looked at sixty-two frail seniors (average age seventy-eight) who engaged in a program of strength training and found that even after six months of pure strength training, half of the subjects did not gain any muscle mass. They also didn’t lose any muscle mass, likely thanks to the weight training, but the upshot is, it is very difficult to put on muscle mass later in life.”
- “Remember the study we discussed in chapter 11 that looked at the effect of strength training in sixty-two frail seniors? The subjects who did only strength training for six months gained no muscle mass. What I didn’t mention there was that another group of subjects was given protein supplementation (via a protein shake); those subjects added an average of about three pounds of lean mass. The extra protein likely made the difference.”
- “A far more important measure of strength, I’ve concluded, is how much heavy stuff you can carry.”
- “still incorporate some kind of carrying, typically with dumbbells, kettlebells, or sandbags, into most of my workouts. I’ve also become semiobsessed with an activity called rucking, which basically means hiking or walking at a fast pace with a loaded pack on your back.”
- “The fifty- to sixty-pound pack on my back makes it quite challenging, so I’m strengthening my legs and my trunk while also getting in a solid cardiovascular session.”
- “(A good goal is to be able to carry one-quarter to one-third of your body weight once you develop enough strength and stamina.”
- “Fundamentally I structure my training around exercises that improve the following: Grip strength, how hard you can grip with your hands, which involves everything from your hands to your lats (the large muscles on your back). Almost all actions begin with the grip. Attention to both concentric and eccentric loading for all movements, meaning when our muscles are shortening (concentric) and when they are lengthening (eccentric). In other words, we need to be able to lift the weight up and put it back down, slowly and with control. Rucking down hills is a great way to work on eccentric strength, because it forces you to put on the “brakes.” Pulling motions, at all angles from overhead to in front of you, which also requires grip strength (e.g., pull-ups and rows). Hip-hinging movements, such as the deadlift and squat, but also step-ups, hip-thrusters, and countless single-leg variants of exercises that strengthen the legs, glutes, and lower back.”
- “A rowing machine, something I love to use for VO2 max training, is another simple and effective way to work on pulling strength.”
Grip Strength
- “Training grip strength is not overly complicated. One of my favorite ways to do it is the classic farmer’s carry, where you walk for a minute or so with a loaded hex bar or a dumbbell or kettlebell in each hand. (Bonus points: Hold the kettlebell up vertically, keeping your wrist perfectly straight and elbow cocked at ninety degrees, as though you were carrying it through a crowded room.)”
- “Another way to test your grip is by dead-hanging from a pull-up bar for as long as you can. (This is not an everyday exercise; rather, it’s a once-in-a-while test set.)””Here we like to see men hang for at least two minutes and women for at least ninety seconds at the age of forty.”
Eccentric Training
- “In life, especially as we age, eccentric strength is where many people falter.”
- “muscles are shortening (concentric) and when they are lengthening (eccentric)”
- “Training eccentric strength is relatively simple. Big picture, it means focusing on the “down” phase of lifts ranging from pull-ups or pull-downs to deadlifts to rows; rucking downhill, carrying a weighted pack, is a great way to build both eccentric strength as well as spatial awareness and control, which are important parts of stability training (next chapter). It also helps protect against knee pain.”
Bone Mineral Density (BMD)
- “Another metric that we track closely in our patients is their bone density (technically, bone mineral density or BMD). We measure BMD in every patient, every year, looking at both of their hips and their lumbar spine using DEXA.”
- “When we detect low or rapidly declining BMD in a middle-aged person, we use the following four strategies: Optimize nutrition, focusing on protein and total energy needs (see nutrition chapters). Heavy loading-bearing activity. Strength training, especially with heavy weights, stimulates the growth of bone—more than impact sports such as running (though running is better than swimming/cycling). Bones respond to mechanical tension and estrogen is the key hormone in mediating the mechanical signal (weight bearing) to a chemical one telling the body to lay down more bone. HRT, if indicated. Drugs to increase BMD, if indicated.”
Chapter 13 – The Gospel of Stability
First, Do Thyself No Harm
- “This is why our approach to exercise must increase not only our conventional measures of fitness, such as our VO2 max and our muscular strength, but above all our resistance to injury.”
- “Studies of college-age athletes who experience injury in their careers find that they report consistently lower quality of life at middle and older ages.”
What is Stability?
- “A technical definition might be: stability is the subconscious ability to harness, decelerate, or stop force. A stable person can react to internal or external stimuli to adjust position and muscular tension appropriately without a tremendous amount of conscious thought.”
- “That’s what stability is about: safe and powerful transmission of force through muscles and bones, and not joints or spinal hinge points.”
- “He doesn’t necessarily look strong. But because he has trained for stability as well as strength, his muscles can transmit much more force across his entire body, from his shoulders to his feet, while protecting his vulnerable back and knee joints. He is like a track-ready race car: strong, fast, stable—and healthy, because his superior stability allows him to do all these things while rarely, if ever, getting injured.”
- Connects with the ideas in Becoming a Supple Leopard by Dr. Kelly Starrett
- “A large part of what we’re working on in stability training is this kind of neuromuscular control, reestablishing the connection between our brain and key muscle groups and joints.”
Dynamic Neuromuscular Stabilization(DNS)
- “The theory behind DNS is that the sequence of movements that young children undergo on their way to learning how to walk is not random or accidental but part of a program of neuromuscular development that is essential to our ability to move correctly.”
- “The only way many of us can come close to matching a toddler’s form is to lie on our backs, as Michael Stromsness demonstrated with me in one of our early sessions. Then it becomes much easier to raise our knees into a perfect squat position, with the correct degree of curvature throughout the spine from the base of the skull to the tailbone. This tells us that range of motion per se is not what’s stopping most adults from squatting well; it’s that when the average adult is under a load, even as little as their own bodyweight, the job of stabilizing his or her own torso becomes too much.”
- “If you’d like to know more after you’ve read this chapter, I suggest visiting the websites for DNS (www.rehabps.com) and the Postural Restoration Institute (PRI) (www.posturalrestoration.com), the two leading exponents of what I’m talking about here.”
- “One simple test that we ask of everyone, early on, looks like this: lie on your back, with one hand on your belly and the other on your chest, and just breathe normally, without putting any effort or thought into it. Notice which hand is rising and falling—is it the one on your chest, or your belly, or both (or neither)?”
- “Making sure that your breath can be wide and three-dimensional and easy is vital for creating good, efficient, coordinated movement,” Beth says.”
- “Be sure to pause after each exhale for at least two counts to hold the isometric contraction—this is key, in DNS.”
- “In DNS, you learn to think of the abdomen as a cylinder, surrounded by a wall of muscle, with the diaphragm on top and the pelvic floor below. When the cylinder is inflated, what you’re feeling is called intra-abdominal pressure, or IAP. It’s critical to true core activation and foundational to DNS training. Learning to fully pressurize the cylinder, by creating IAP, is important to safe movement because the cylinder effectively stabilizes the spine.”
- “It’s as if you have a plastic bottle: with the cap off, you can crush the bottle in one hand; with the cap on, there is too much pressure (i.e., stability) and the bottle can’t be crushed.”
- Squats : “Beth typically has someone like me hold a weight in front of my body, a few inches in front of the sternum.”
Feet Stuff
- “If the road to stability begins with the breath, it travels through the feet—the most fundamental point of contact between our bodies and the world. Our feet are literally the foundation for any movement we might make.”
- “Toe yoga is a lot harder than it sounds, which is why I’ve posted a video demonstration of this and other exercises at www.peterattiamd.com/outlive/videos“
- “First, Beth tells her students to think of their feet as having four corners, each of which needs to be rooted firmly on the ground at all times, like the legs of a chair. As you stand there, try to feel each “corner” of each foot pressing into the ground: the base of your big toe, the base of your pinky toe, the inside and outside of your heel.”
- “Beth compares pronation to driving a car with too little air in the tires, meaning you kind of slosh through your movements, unable to transfer force efficiently to the ground. Supination, on the other hand, is like having overinflated tires, so you skid and bounce around. Your feet are unable to absorb shock, and all that bouncing and jarring gets transferred straight to the ankles, hips, knees, and lower back.”
- “I prefer to lift barefoot or in minimal shoes, with little to no cushioning in the soles because it allows me feel the full surface of my feet at all times.)”
- “One key test in our movement assessment is to have our patients stand with one foot in front of the other and try to balance. Now close your eyes and see how long you can hold the position. Ten seconds is a respectable time; in fact, the ability to balance on one leg at ages fifty and older has been correlated with future longevity, just like grip strength. (Pro tip: balancing becomes a lot easier if you first focus on grounding your feet, as described above.)”
Posture & Exercises
- “The spine has three parts: lumbar (lower back), thoracic (midback), and cervical (neck) spine. Radiologists see so much degeneration in the cervical spine, brought on by years of hunching forward to look at phones, that they have a name for it: “tech neck.””
- “Beth taught me a simple exercise to help understand the importance of scapular positioning and control, a movement known as Scapular CARs, for controlled articular rotations: Stand with your feet shoulder-width apart and place a medium to light resistance band under your feet, one handle in each hand (a very light dumbbell also works).”
- “There is a strong correlation between having a weak rotator cuff (shoulder) and weak grip strength.”
- “one of the key things Beth taught me is that a deadlift is as much about feet and hands as hamstrings and glutes. We’re pushing the floor away as we lift with our fingers.”
- “The “Barry Get-Up” has become a key part of the fitness assessment that we do with all our patients, as well as one of the key events in the Centenarian Decathlon (it should be in yours, too). It’s an important move, whether you’re picking yourself up off the ground after a stumble or playing with grandchildren on the floor. (For a video demonstration of the Barry Get-Up, please visit www.peterattiamd.com/outlive/videos.)”
It gives us the ability to pick ourselves up off the ground—literally and figuratively—and become stronger and more capable. It’s not about slowing the decline, it’s about getting better, and better, and better.
PETER ATTIA – OUTLIVE
Chapter 14 – Nutrition 3.0
There are forty thousand diet books on Amazon; they can’t all be right.
PETER ATTIA – OUTLIVE
Religion is a culture of faith; science is a culture of doubt.
Richard Feynman
- “Richard Feynman being asked at a party to explain, briefly and simply, why he was awarded his Nobel Prize. He responded that if he could explain his work briefly and simply, it probably would not have merited a Nobel Prize.”
- “The fundamental assumption underlying the diet wars, and most nutrition research—that there is one perfect diet that works best for every single person—is absolutely incorrect.”
- “Instead of diet, we should be talking about nutritional biochemistry. That takes it out of the realm of ideology and religion—and above all, emotion—and places it firmly back into the realm of science. We can think of this new approach as Nutrition 3.0: scientifically rigorous, highly personalized, and (as we’ll see) driven by feedback and data rather than ideology and labels. It’s not about telling you what to eat; it’s about figuring out what works for your body and your goals—and, just as important, what you can stick to.”
- “But I also believe that we need to differentiate between behavior that maintains good health versus tactics that correct poor health and disease. Wearing a cast on a broken bone will allow it to heal. Wearing a cast on a perfectly normal arm will cause it to atrophy.”
- “It seems quite clear that a nutritional intervention aimed at correcting a serious problem (e.g., highly restricted diets, even fasting, to treat obesity, NAFLD, and type 2 diabetes) might be different from a nutritional plan calibrated to maintain good health (e.g., balanced diets in metabolically healthy people).”
- “Nutrition is relatively simple, actually. It boils down to a few basic rules:
- don’t eat too many calories, or too few;
- consume sufficient protein and essential fats;
- obtain the vitamins and minerals you need;
- and avoid pathogens like E. coli and toxins like mercury or lead.
- Beyond that, we know relatively little with complete certainty.”
- “Hill had helped sleuth out the link between smoking and lung cancer in the early 1950s, and he came up with nine criteria for evaluating the strength of epidemiological findings and determining the likely direction of causality, which we also referenced in regard to exercise.[*3]”
- “strength of association, consistency, specificity, temporality, biological gradient, plausibility, coherence, experiment, and analogy” (Source)
- “So do red and processed meats actually cause cancer or not? We don’t know, and we will probably never get a more definitive answer, because a clinical trial testing this proposition is unlikely ever to be done. Confusion reigns. Nevertheless, I’m going to stick my neck out and assert that a risk ratio of 1.17 is so minimal that it might not matter that much whether you eat red/processed meats versus some other protein source, like chicken.”
- “The low-calorie mice were found to live the longest, followed by medium-calorie mice, and the high-calorie mice lived the shortest, on average. This was the expected result that had been well established in many previous studies. But then Allison did something very clever. He looked more closely at the high-calorie group, the mice with no maximum limit on food intake, and analyzed this group separately, as its own nonrandomized epidemiological cohort. Within this group, Allison found that some mice chose to eat more than others—and that these hungrier mice actually lived longer than the high-calorie mice who chose to eat less. This was exactly the opposite of the result found in the larger, more reliable, and more widely repeated randomized trial. There was a simple explanation for this: the mice that were strongest and healthiest had the largest appetites, and thus they ate more.”
- “the people who are still drinking in older age tend to do so because they are healthy, and not the other way around. Similarly, people who drink zero alcohol often have some health-related reason, or addiction-related reason, for avoiding it. And such studies also obviously exclude those who have already died of the consequences of alcoholism.”
- “But a recent study in JAMA, using the tool of Mendelian randomization we discussed back in chapter 3, suggests that this might not be true. This study found that once you remove the effects of other factors that may accompany moderate drinking—such as lower BMI, affluence, and not smoking—any observed benefit of alcohol consumption completely disappears. The authors concluded that there is no dose of alcohol that is “healthy.””
- “There’s a trade-off between sample size, study duration, and control.”
- “In fact, I’m convinced that compliance is the key issue in nutrition research, and with diets in general: Can you stick to it? The answer is different for almost everyone.”
Efficacy tests how well the intervention works under perfect conditions and adherence (i.e., if one does everything exactly as prescribed). Effectiveness tests how well the intervention works under real-world conditions, in real people.
PETER ATTIA – OUTLIVE
Chapter 15 – Putting Nutritional Biochemistry into Practice
In the end, the best nutrition plan is the one that we can sustain. How you manipulate the three levers of diet—calorie restriction, dietary restriction, and time restriction—is up to you. Ideally, your plan improves or maintains all the parameters we care about—not only blood glucose and insulin but also muscle mass and lipid levels, and possibly even weight—while reducing your risk of your most proximate Horseman or Horsemen.
PETER ATTIA – OUTLIVE
Bad nutrition can hurt us more than good nutrition can help us. If you’re already metabolically healthy, nutritional interventions can only do so much.
PETER ATTIA – OUTLIVE
The 3 Levers
- “CALORIC RESTRICTION, or CR: eating less in total, but without attention to what is being eaten or when it’s being eaten
- DIETARY RESTRICTION, or DR: eating less of some particular element(s) within the diet (e.g., meat, sugar, fats)
- TIME RESTRICTION, or TR: restricting eating to certain times, up to and including multiday fasting…”
Visualize the three levers in this article.
The patient has not failed the treatment; the treatment has failed the patient. These patients needed a different treatment.
PETER ATTIA – OUTLIVE
Caloric Restriction – CR
- “If this imbalance continues, we exceed the capacity of our “safe” subcutaneous fat tissue, and excess fat spills over into our liver, our viscera, and our muscles.”
- “In the end, the calorically restricted monkeys lived significantly longer and proved far less likely to die of age-related diseases than the ad libitum–fed control monkeys. They were healthier by many other measures, such as insulin sensitivity. Even their brains were in better shape than those of the controls, retaining more gray matter as they aged. “These data demonstrate that caloric restriction slows aging in a primate species,” the study authors concluded.”
- “The Wisconsin animals ate an off-the-shelf commercial monkey chow that was “semipurified,” meaning its ingredients were highly processed and rigorously titrated. The NIH monkeys were fed a diet that was similar in its basic macronutrient profile, but their chow was “natural” and less refined, custom formulated from whole ingredients by an in-house primate nutritionist at NIH. The most glaring contrast: while the NIH monkey chow contained about 4 percent sugar, the Wisconsin diet comprised an astonishing 28.5 percent sucrose, by weight. That is a greater proportion of sugar than you’ll find in vanilla Häagen-Dazs ice cream. Could that alone have explained the difference in survival outcomes? Possibly: more than 40 percent of the Wisconsin control monkeys, the ones not subject to calorie limitations, developed insulin resistance and prediabetes, while just one in seven of the NIH controls became diabetic.[*1] And the Wisconsin control monkeys proved far more likely to die from cardiovascular causes and cancer than monkeys from any other group. This could suggest that caloric restriction was eliminating early deaths because of the bad Wisconsin diet more than it was actually slowing aging”
- “Taken together, then, what do these two monkey studies have to tell us about nutritional biochemistry? Avoiding diabetes and related metabolic dysfunction—especially by eliminating or reducing junk food—is very important to longevity. There appears to be a strong link between calories and cancer, the leading cause of death in the control monkeys in both studies. The CR monkeys had a 50 percent lower incidence of cancer. The quality of the food you eat could be as important as the quantity. If you’re eating the SAD, then you should eat much less of it. Conversely, if your diet is high quality to begin with, and you are metabolically healthy, then only a slight degree of caloric restriction—or simply not eating to excess—can still be beneficial.”
- “if you are eating a higher-quality diet—and are metabolically healthy to begin with—then severe caloric restriction may not even be necessary. The NIH control monkeys ate as much as they wanted of their better diet and still lived nearly as long as the CR monkeys in both studies. Interestingly, the post facto analyses also revealed that the NIH control monkeys naturally consumed about 10 percent fewer calories per day than the Wisconsin controls, likely because their higher-quality diet left them feeling less hungry.”
Dietary Restriction – DR
- “There is ample evidence to suggest that they were opportunistic omnivores, out of necessity. They ate anything and everything they could get their hands on: lots of plants, lots of starch, animal protein whenever they could, honey and berries whenever possible. They also seemed to be, at least on the basis of the study of the few remaining hunter-gatherer societies, very metabolically healthy.”
- “Even if done correctly and strictly, DR can still result in overnutrition. If you cut out carbohydrates altogether but overdo it on the Wagyu steaks and bacon, you will fairly easily find yourself in a state of caloric excess. The key is to pick a strategy to which you can adhere but that also helps achieve your goals. This takes patience, some willpower, and a willingness to experiment.”
- “Similar diets yield very different outcomes, depending on the individual.”
- “The way we do this is by manipulating our four macronutrients: alcohol, carbohydrates, protein, and fat. How well do you tolerate carbohydrates? How much protein do you require? What sorts of fats suit you best? How many calories do you require each day? What is the optimal combination for you?”
- “It’s easy to overlook, but alcohol should be considered as its own category of macronutrient because it is so widely consumed, it has such potent effects on our metabolism, and it is so calorically dense at 7 kcal/g (closer to the 9 kcal/g of fat than the 4 kcal/g of both protein and carbohydrate).”
Continuous Glucose Monitor – CGM
It is important to remember the limitations of CGM—chiefly, that it measures one variable. This variable happens to be very important, but it is not the only one. … Similarly, a bathroom scale will suggest that smoking is good for you because you lost weight.
PETER ATTIA – OUTLIVE
- “But there is also evidence suggesting that repeated blood glucose spikes, and the accompanying rise(s) in insulin, may have negative consequences in and of themselves.”
- “CGM costs about $120 a month, which is not insignificant—but I would argue that even this is still far cheaper than allowing someone to slide into metabolic dysfunction and eventually type 2 diabetes. Insulin treatment alone can cost hundreds of dollars a month.”
- “The second argument against using CGM in healthy patients is also pretty typical: There are no randomized clinical trials showing a benefit from the technology.”
- “I am confident that such studies will show a benefit, if done correctly, because there are already ample data showing how important it is to keep blood glucose low and stable. A 2011 study looking at twenty thousand people, mostly without type 2 diabetes, found that their risk of mortality increased monotonically with their average blood glucose levels (measured via HbA1c). The higher their blood glucose, the greater their risk of death—even in the nondiabetic range of blood glucose. Another study in 2019 looked at the degree of variation in subjects’ blood glucose levels and found that the people in the highest quartile of glucose variability had a 2.67 times greater risk of mortality than those in the lowest (most stable) quartile. From these studies, it seems quite clear that we want to lower average blood glucose and reduce the amount of variability from day to day and hour to hour.”
- “When I’ve put my patients on CGM, I’ve observed that there are two distinct phases to the process.
- The first is the insight phase, where you learn how different foods, exercise, sleep (especially lack thereof), and stress affect your glucose readings in real time. The benefit of this information can’t be overstated. Almost always, patients are stunned to see how some of their favorite foods send their glucose soaring, then crashing back to earth.
- This leads to the second phase, which is what I call the behavior phase. Here you mostly know how your glucose is going to respond to that bag of potato chips, and that knowledge is what prevents you from mindlessly eating it. I’ve found that CGM powerfully activates the Hawthorne effect, the long-observed phenomenon whereby people modify their behavior when they are being watched. (The Hawthorne effect is also what makes it difficult to study what people actually eat, for the same reason.)”
- “CGM has proved especially useful in patients with APOE e4, where we often see big glucose spikes, even in relatively young people. In these patients, the behavior modification that CGM prompts is an important part of their Alzheimer’s disease prevention strategy.”
- “Overall, I like to keep average glucose at or below 100 mg/dL, with a standard deviation of less than 15 mg/dL.[*5] These are aggressive goals: 100 mg/dL corresponds to an HbA1c of 5.1 percent.”
- “Also, everyone tends to be more insulin sensitive in the morning than in the evening, so it makes sense to front-load our carb consumption earlier in the day.”
- “One thing CGM pretty quickly teaches you is that your carbohydrate tolerance is heavily influenced by other factors, especially your activity level and sleep.”
- “A good versus bad night of sleep makes a world of difference in terms of glucose control. All things equal, it appears that sleeping just five to six hours (versus eight hours) accounts for about a 10 to 20 mg/dL (that’s a lot!) jump in peak glucose response, and about 5 to 10 mg/dL in overall levels.”
- “If she goes to bed at, say, 80 mg/dL, but then her glucose ramps up to 110 for most of the night, that tells me that she is likely dealing with psychological stress.”
- “This doesn’t need to be an exercise in deprivation: one patient of mine gleefully confessed that his CGM, which he had only reluctantly agreed to wear, had given him a “superpower” to cheat. By eating certain “forbidden” types of carbohydrates only at certain times, either mixed with other foods or after exercising, he had figured out how he could hit his average glucose goals while still enjoying all the foods he loved.”
- “Fructose does not get measured by CGM, but because fructose is almost always consumed in combination with glucose, fructose-heavy foods will still likely cause blood-glucose spikes.”
- “Perhaps the most important insight of them all? Simply tracking my glucose has a positive impact on my eating behavior. I’ve come to appreciate the fact that CGM creates its own Hawthorne effect, a phenomenon where study subjects change their behavior because they are being observed.”
Protein
- “Unlike carbs and fat, protein is not a primary source of energy. We do not rely on it in order to make ATP,[*8] nor do we store it the way we store fat (in fat cells) or glucose (as glycogen). If you consume more protein than you can synthesize into lean mass, you will simply excrete the excess in your urine as urea.”
- Analogous to burning furniture for heat. Much more efficient to burn raw fire wood.
- “While carbohydrates are primarily a source of fuel and amino acids are primarily building blocks, fats are both. They are very efficient fuel for oxidation (think: slow-burning logs) and also the building blocks for many of our hormones (in the form of cholesterol) and cell membranes.”
- “The first thing you need to know about protein is that the standard recommendations for daily consumption are a joke. Right now the US recommended dietary allowance (RDA) for protein is 0.8 g/kg of body weight. This may reflect how much protein we need to stay alive, but it is a far cry from what we need to thrive. There is ample evidence showing that we require more than this—and that consuming less leads to worse outcomes. More than one study has found that elderly people consuming that RDA of protein (0.8 g/kg/day) end up losing muscle mass, even in as short a period as two weeks. It’s simply not enough.”
- “How much protein do we actually need? It varies from person to person. In my patients I typically set 1.6 g/kg/day as the minimum, which is twice the RDA. The ideal amount can vary from person to person, but the data suggest that for active people with normal kidney function, one gram per pound of body weight per day (or 2.2 g/kg/day) is a good place to start—nearly triple the minimal recommendation. So if someone weighs 180 pounds, they need to consume a minimum of 130 grams of protein per day, and ideally closer to 180 grams, especially if they are trying to add muscle mass.”
- “added challenge is that it should not be taken in one sitting but rather spread out over the day to avoid losing amino acids to oxidation.”
- “Eating protein also helps us feel satiated, inhibiting the release of the hunger-inducing hormone ghrelin, so we eat fewer calories overall.”
Fats
- “There are (broadly) three types of fats: saturated fatty acids (SFA), monounsaturated fatty acids (MUFA), and polyunsaturated fatty acids (PUFA).[*9]”
- “The key thing to remember—and somehow this is almost always overlooked—is that virtually no food belongs to just one group of fats.”
- “From our empirical observations and what I consider the most relevant literature, which is less than perfect, we try to boost MUFA closer to 50–55 percent, while cutting SFA down to 15–20 percent and adjusting total PUFA to fill the gap. We also boost EPA and DHA, those fatty acids that are likely important to brain and cardiovascular health, with marine fat sources and/or supplementation.”
- “As we discussed in the introduction to Medicine 3.0 and earlier in this chapter, any hope of using broad insights from evidence-based medicine is bound to fail when it comes to nutrition, because such population-level data cannot provide much value at the individual level when the effect sizes are so small, as they clearly are here. All Medicine 2.0 has to offer is broad contours: MUFA seems to be the “best” fat of the bunch (based on PREDIMED and the Lyon Heart study), and after that the meta-analyses suggest PUFA has a slight advantage over SFA. But beyond that, we are on our own.”
- “Subtle changes in fat intake, particularly of saturated fats, can make a significant difference in lipid levels in some people, as I have learned over and over again—but not in others. Some people (like me)[*13] can consume saturated fats with near impunity, while others can hardly even look at a slice of bacon without their apoB number jumping to the 90th percentile.”
- “In the final analysis, I tell my patients that on the basis of the least bad, least ambiguous data available, MUFAs are probably the fat that should make up most of our dietary fat mix, which means extra virgin olive oil and high-MUFA vegetable oils. After that, it’s kind of a toss-up, and the actual ratio of SFA and PUFA probably comes down to individual factors such as lipid response and measured inflammation. Finally, unless they are eating a lot of fatty fish, filling their coffers with marine omega-3 PUFA, they almost always need to take EPA and DHA supplements in capsule or oil form.”
Time Restriction – TR
- “In my experience, most people find this to be the easiest way to reduce their caloric intake, by focusing on when they are eating rather than how much and/or what they are eating. But I am not convinced that short-term time-restricted feeding has much of a benefit beyond this.”
- “Time-restricted feeding is a way of putting the brakes on snacking and late-night meals—the type of mindless eating-just-to-eat that the Japanese call kuchisabishii, for “lonely mouth.””
- “One not uncommon scenario that we see with TR is that a person loses weight on the scale, but their body composition alters for the worse: they lose lean mass (muscle) while their body fat stays the same or even increases.”
- “Because a mouse lives for only about two to three years—and will die after just forty-eight hours without food—a sixteen-hour fast for a mouse is akin to a multiday fast for a human. It’s just not a valid comparison. Human trials of this eating pattern have failed to find much of a benefit.”
- “As a result of this and other research, I have become convinced that frequent, prolonged fasting may be neither necessary nor wise for most patients. The cost, in terms of lost lean mass (muscle) and reduced activity levels, simply does not justify whatever benefits it may bring.”
Chapter 16 – The Awakening
There I was again, bravely ascending the flanks of Mount Stupid. But Kirk stopped me short with a simple, Socratic question. If sleep is so unimportant, he asked, then why hasn’t evolution gotten rid of it?
PETER ATTIA – OUTLIVE
Sleep Benefits
- “We need to sleep about seven and a half to eight and a half hours a night. There is even some evidence, from studies conducted in dark caves, that our eight-ish-hour sleep cycle may be hard-wired to some extent, suggesting that this requirement is non-negotiable.”
- “No fewer than nine different studies have found that sleep deprivation increases insulin resistance by up to a third.”
- “From years of experience with my own CGM and that of my patients, it still amazes me how much even one night of horrible sleep cripples our ability to dispose of glucose the next day.”
- “high overnight glucose on CGM is almost always a sign of excessive cortisol, sometimes exacerbated by late-night eating and drinking. If it persists, this elevated blood glucose can lead to type 2 diabetes.”
- “People who sleep eleven hours or more nightly have a nearly 50 percent higher risk of all-cause mortality, likely because long sleep = poor quality sleep, but it may also reflect an underlying illness.”
- “Studies by Eve van Cauter’s group have found that limiting subjects’ sleep to four or five hours a night suppresses their levels of leptin, the hormone that signals to us that we are fed, while increasing levels of ghrelin, the “hunger” hormone. When we sleep poorly, we can be desperately, irrationally hungry the next day, and more likely to reach for high-calorie and sugary foods than their healthy alternatives.”
- “Follow-up studies by van Cauter’s group have found that short-sleeping subjects ate about three hundred extra calories’ worth of food the following day, compared with when they were well rested.”
- “Researchers have observed a direct, linear relationship between how much deep sleep we get in a given night and how well we will perform on a memory test the next day.”
- “This cleansing process flushes out detritus, including both amyloid-beta and tau, the two proteins linked to neurodegeneration. But if we do not spend enough time in deep sleep, the system cannot work as effectively, and amyloid and tau build up among the neurons. Broader studies have found that people who have generally slept less than seven hours per night, over decades, tend to have much more amyloid-beta and tau built up in their brains than people who sleep for seven hours or more per night. Tau, the protein that collects in “tangles” inside unhealthy neurons, is itself correlated to sleep disturbances in cognitively normal people and in those with MCI, or mild cognitive impairment, an early stage of dementia.”
Sleep Meds
- “One study found that Ambien actually decreased slow-wave sleep (deep sleep) without increasing REM, meaning people who take it are basically trading high-quality sleep for low-quality sleep.”
- “If they are using Ambien or Xanax once a month, or only with travel, or to help them sleep during a time of emotional distress, it’s not alarming. But if they are using such drugs regularly, it becomes our highest priority to get them off these sleep aids and have them begin to learn to sleep correctly without them.”
- “One drug that we do find helpful for assisting with sleep is trazodone, a fairly old anti-depressant (approved in 1981) that never really took off. At the doses used to treat depression, two hundred to three hundred milligrams per day, it had the unwanted side effect of causing users to fall asleep. But one man’s trash is another man’s treasure. That side effect is what we want in a sleep medication, especially if it also improves sleep architecture, which is exactly what trazodone does—and most other sleep meds do not.[*4] We typically use it at much lower doses, from one hundred milligrams down to fifty milligrams or even less; the optimal dosing depends on the individual, but the goal is to find the amount that improves their sleep quality without next-day grogginess. (We have also had good results with the supplement ashwagandha.)”
Insomnia
- “Studies of CBT-I techniques have found that they are more effective than sleeping medications.”
- “The key, says Vikas Jain, is to find something that is relaxing and enjoyable but that serves no function; you never want to give your insomnia a purpose, such as doing work or paying bills, because if you do, your brain will make sure to wake you up for it on a regular basis.”
Sleep Protocol
The overarching point here is that a good night of sleep may depend in part on a good day of wakefulness: one that includes exercise, some outdoor time, sensible eating (no late-night snacking), minimal to no alcohol, proper management of stress, and knowing where to set boundaries around work and other life stressors.
PETER ATTIA – OUTLIVE
- Limit interactive devices before bed.
- “One large-scale survey found that the more interactive devices subjects used during the hour before bedtime, the more difficulties they had falling asleep and staying asleep—whereas passive devices such as TV, electronic music players, and, best of all, books were less likely to be associated with poor sleep. This may partially explain why watching TV before bed does not seem to affect sleep quite as negatively as playing video games or scrolling social media does, according to research by Michael Gradisar, a sleep researcher and professor of psychology at Flinders University in Australia.”
- “Turn off the computer and put away your phone at least an hour before bedtime. Do NOT bring your laptop or phone into bed with you.”
- Keep your bedroom cool.
- “around sixty-five degrees Fahrenheit seems to be optimal. A warm bath before bed may actually help with this process, not only because the bath itself is relaxing but also because when we get out of the bath and climb into our cool bed, our core temperature drops, which signals to our brain that it is time to fall asleep. (There are also a variety of cooling mattresses and mattress toppers out there that could help people who like to sleep cool.)”
- Limit caffeine.
- “Everyone differs in their caffeine tolerance, based on genes and other factors (23andMe tests for one common caffeine-related gene).”
- Accumulate sleep pressure.
- “This is why one of the primary techniques that doctors use to treat patients with insomnia is actually sleep restriction, limiting the hours when they are “allowed” to sleep to six, or less. This basically makes them tired enough that they fall asleep more easily at the end of the day, and (hopefully) their normal sleep cycle is restored. Their sleep pressure builds up to the point where it overwhelms whatever is causing their insomnia. But this also helps explain why napping can be counterproductive.”
- “Another way to help cultivate sleep pressure is via exercise, particularly sustained endurance exercise (e.g., zone 2), ideally not within two or three hours of bedtime.”
- Expose yourself to sunlight outdoors.
- Meditation or NSDR
- Get hot to get cold.
- “For folks who have access, spend time in a sauna or hot tub prior to bed. Once you get into the cool bed, your lowering body temperature will signal to your brain that it’s time to sleep. (A hot bath or shower works too.)”
- Get dark.
- “If that is not achievable, use an eye shade. I use a silky one called Alaska Bear that costs about $8 and works better than the fancier versions I’ve tried.”
- Stay the course.
- “Fix your wake-up time—and don’t deviate from it, even on weekends. If you need flexibility, you can vary your bedtime, but make it a priority to budget for at least eight hours in bed each night.”
- Get loose.
- “Don’t obsess over your sleep, especially if you’re having problems. If you need an alarm clock, make sure it’s turned away from you so you can’t see the numbers. Clock-watching makes it harder to fall asleep. And if you find yourself worrying about poor sleep scores, give yourself a break from your sleep tracker.”
Chapter 17 – Work in Progress
Why would you want to live longer if you’re so unhappy?
Esther Perel
Why Care About Emotions?
- “This is why I’ve come to believe that emotional health may represent the most important component of healthspan. Nothing else about longevity is really worth much without some degree of happiness, fulfillment, and connection to others. And misery and unhappiness can also destroy your physical health, just as surely as cancer, heart disease, neurodegenerative disease, and orthopedic injury.”
90% of male rage is helplessness masquerading as frustration.
Terrence Real – I Don’t Want to Talk about it
Wrecking Ball
- “In early November, a woman from the Bridge called to do my intake interview. It was a long, tedious conversation, and my patience finally expired when she asked, “Have you ever been subject to any kind of abuse?” I got so angry I yelled, “Fuck you!” and hung up the phone. After this call I decided to cancel my planned stay.”
- “Whenever I made a mistake or felt I performed poorly, even in tiny ways, my own personal Coach Knight jumped up from the bench to scream at me. Make a mistake cooking dinner? How do you not know how to grill a fucking steak? Flub the intro recording to a podcast? You are a worthless sack of shit who has no business being alive, let alone having a podcast! The crazy part is that I actually believed that voice served me well. This rage and self-doubt had fueled much of my personal drive and whatever success I had enjoyed, I told myself. It was simply the price I had to pay. But in reality, all it had produced was more résumé virtues. And I wasn’t even all that proud of my résumé. It would never be good enough. For the first time in my life, I had a radical thought: Who cares how well you perform if you’re so utterly miserable?”
- “And just like that, I spun into a radical, self-destructive episode, one like I’ve never experienced before or since. Even remembering it now is terrifying. I threw a table across our living room. I tore my T-shirt to pieces. I screamed, in rage and pain. My wife begged me to leave the house for fear I would harm her or the kids. I thought about driving myself into a bridge abutment or other structure fast enough that I’d be killed. I was convinced that I was broken, defective; when they autopsied my brain, they would discover just how screwed up I was. I was beyond fixing. Nothing could make it right.”
- “On my second day, I was assigned to write out a list of forty-seven affirmations, representing one positive statement about myself for each year of my life. I made it to about five or six before I got completely stuck. For days and days, I couldn’t come up with anything good to say about myself. My perfectionism and my shame did not permit me to believe anything nice about myself. I just couldn’t do it.”
- “It had been two and a half years in the making, but I finally was able to let go and accept the truth about my past and how it had shaped me, without any excuses or rationalizations. All that I had become—good and bad—was in response to what I had experienced. It wasn’t simply the big-T traumas, either; we uncovered many, many more little-t traumas, hidden in the cracks, that had affected me even more profoundly. I hadn’t been protected. I hadn’t felt safe. My trust had been broken by people who were close to me. I felt abandoned. All of that had manifested itself as my own self-loathing as an adult; I had become my own worst enemy. And I hadn’t deserved any of it. This was the key insight. That little, sweet boy did not deserve any of it. And he was still with me.”
- “What I eventually realized, after this long and very painful journey, is that longevity is meaningless if your life sucks. Or if your relationships suck. None of it matters if your wife hates you. None of it matters if you are a shitty father, or if you are consumed by anger or addiction. Your résumé doesn’t really matter, either, when it comes time for your eulogy.”
“Family pathology rolls from generation to generation like a fire in the woods taking down everything in its path until one person, in one generation, has the courage to turn and face the flames. That person brings peace to his ancestors and spares the children that follow.” I wanted to be that person.
Trauma
- “Trauma generally falls into five categories: (1) abuse (physical or sexual, but also emotional or spiritual); (2) neglect; (3) abandonment; (4) enmeshment (the blurring of boundaries between adults and children); and (5) witnessing tragic events. Most of the things that wound children fit into these five categories.”
- “Trauma is a pretty loaded word, and the therapists at the Bridge were careful to explain that there can be “big-T” trauma or “little-t” traumas. Being a victim of rape would qualify as a big-T trauma, while having an alcoholic parent might subject a child to a host of little-t traumas. But in large enough doses over a long enough time, little-t traumas can shape a person’s life just as much as one major terrible event. Both types can do tremendous damage, but little-t trauma is more challenging to address—in part, I suspect, because we are more inclined to dismiss it.”
- “Trauma, big T or little t, means having experienced moments of perceived helplessness. The situations in question may or may not have been life-or-death, he explained, “but to a child with an undeveloped brain, it may have seemed that way.””
- “There are many rules at the Bridge, and one of the most important ones is no minimizing. You are not allowed to minimize anything that someone else is saying, and you are especially not allowed to minimize your own experiences. But she didn’t flag me for that. Instead, she asked a simple question: “You were five years old when this first happened to you, right?” “That’s right,” I replied. “And your son Reese is almost five years old now, right?” I nodded. “So you’re saying it’s okay that this happened to you when you were his age—but would you be okay with people doing that to Reese now?””
- “There is no bright line between trauma and adversity; terrible as it was, my own experience had made me stronger in some ways. Julie’s question is a pretty good litmus test: Would I want my child to experience it?”
- “This dysfunction is represented by the four branches of the trauma tree: (1) addiction, not only to vices such as drugs, alcohol, and gambling, but also to socially acceptable things such as work, exercise, and perfectionism (check); (2) codependency, or excessive psychological reliance on another person; (3) habituated survival strategies, such as a propensity to anger and rage (check); (4) attachment disorders, difficulty forming and maintaining connections or meaningful relationships with others (check).”
- “At the Bridge, I learned that children don’t respond to a parent’s anger in a logical way. If they see me screaming at a driver who just cut me off, they internalize that rage as though it were directed to them. Second, trauma is generational, although not necessarily linear. Children of alcoholics are not inevitably destined to become alcoholics themselves, but one way or another, trauma finds its way down the line.”
Religion is for people who are afraid of Hell. Spirituality is for people who have been there.
Recovery
- “It reminded me of this observation by Jacob Riis, the great Danish American journalist and social reformer: “When nothing seems to help, I go back and look at a stonecutter hammering away at his rock perhaps a hundred times without as much as a crack showing in it. Yet at the hundred-and-first blow it will split in two, and I know it was not the last blow that did it, but all that had gone before.””
- “True recovery requires probing the depths of what shaped you, how you adapted to it, and how those adaptations are now serving you (or not, as in my case).”
Dialectical Behaviour Therapy – DBT
- “DBT was developed to help individuals with more serious and potentially dangerous issues, such as an inability to regulate their emotions and a propensity to harm themselves or even attempt suicide. These people are lumped into something called borderline personality disorder, which is a bit of a catch-all diagnosis, but DBT has also been found to be helpful in patients with less dramatic and dangerous emotional health issues, a category that encompasses many more of us.”
- “The practice of DBT is predicated on learning to execute concrete skills, repetitively, under stress, that aim to break the chain reaction of negative stimulus → negative emotion → negative thought → negative action.”
- “DBT consists of four pillars joined by one overarching theme. The overarching theme is mindfulness, which gives you the ability to work through the other four: emotional regulation (getting control over our emotions), distress tolerance (our ability to handle emotional stressors), interpersonal effectiveness (how well we make our needs and feelings known to others), and self-management (taking care of ourselves, beginning with basic tasks like getting up in time to go to work or school).”
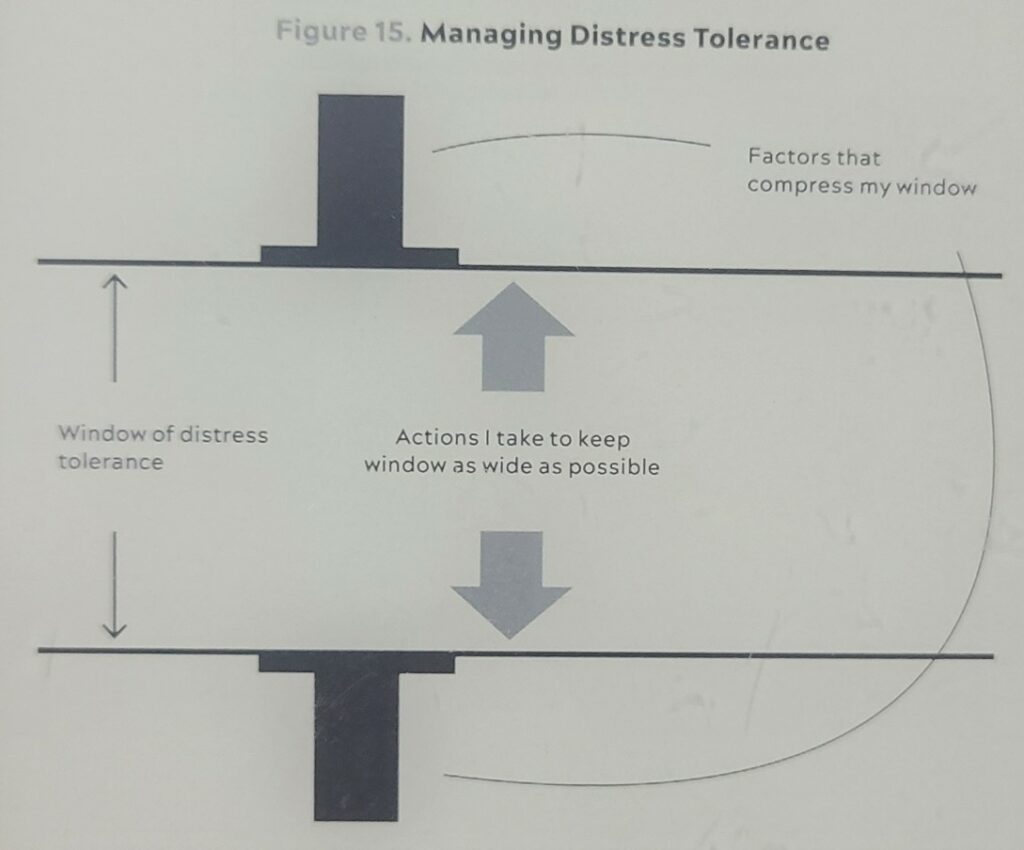
Behavioural Interventions
- “Many behaviors expand this window: exercise, sound sleep, good nutrition, time with my family, medications such as antidepressants or mood stabilizers, deep social connections, spending time in nature, and recreational activities that do not emphasize self-judgment. These are the things I have control over. I don’t have as much control over the things that compress my window, but I still have some—for example, overcommitting to projects and saying yes to more than I should.”
- “That gap, in turn, allows us to process the situation in a calmer and more rational way. Do we really need to honk and curse, and potentially make the situation worse (even if the guy deserves it)? Or is it better to simply accept what happened and move on? Mindfulness helps us reframe it: The other driver may be rushing to the hospital with a sick child, for all we know.”
- “As the breath goes, the nervous system follows.”
- “One tactic that I’ve found especially helpful is called opposite action—that is, if I feel like doing one thing (generally, not a helpful or positive thing), I’ll force myself instead to do the exact opposite. By doing so, I also change the underlying emotions.”
- “changing the behavior can change the mood. You do not need to wait for your mood to improve to make a behavior change. This is also why cognitive therapies alone sometimes come up short; simply thinking about problems might not help if our thinking itself is disordered.”
- “Exercise is another important component of my overall emotional health program, particularly my practice of rucking, discussed in chapter 12. I find that spending time moving in nature, simply enjoying the feeling of the wind in my face and the smell of the budding spring leaves (and a heavily loaded pack on my back) helps me cultivate what Ryan Holiday calls “stillness,” the ability to remain calm and focused amid all the distractions that our world offers and that we create for ourselves.”
- “And as Michael Easter pointed out to me, there is actual research suggesting that exposing oneself to the fractal geometric patterns in nature can reduce physiological stress, and that these effects show up on an EEG.”
Individual Therapy
- “The most important “tactic” by far is my regular weekly therapy session (down from three or four per week when I left PCS).”
- “I feel strongly that there is no substitute for this kind of work with a trained therapist.”
- “This is the key step. You have to believe you can change—and that you deserve better.”
Maybe the journey isn’t so much about becoming anything. Maybe it’s about unbecoming everything that isn’t really you, so you can be who you were meant to be in the first place.
Paulo Coelho
Potential Action Steps
- Habits
- Sleep
- Strength training (Peter’s videos)
- Zone 2 Cardio (three hours per week of zone 2, or four 45-minute sessions)
- VO2 Max
- Floss (reduce inflammation for Alzheimer’s)
- Mediterranean diet seems to work well for me and many folks.
- Saunas
- Take advantage of all my benefits from work. Book and schedule them at the start of each year.
- Not drink or smoke
- Avoid injuries
- Body Composition:
- DEXA scan to check for visceral fat.
- Buy a smart scale that syncs with my Fitbit.
- Blood Test:
- Uric acid
- Oral glucose tolerance test (OGTT)
- apoB
- Lp(a)
- “In my patients, I monitor several biomarkers related to metabolism, keeping a watchful eye for things like elevated uric acid, elevated homocysteine, chronic inflammation, and even mildly elevated ALT liver enzymes. Lipoproteins, which we will discuss in detail in the next chapter, are also important, especially triglycerides; I watch the ratio of triglycerides to HDL cholesterol (it should be less than 2:1 or better yet, less than 1:1), as well as levels of VLDL, a lipoprotein that carries triglycerides—all of which may show up many years before a patient would meet the textbook definition of metabolic syndrome.”
- Genetics Test:
- APOE e4 (Alzeimers)
- Cancer Screening:
- Colonoscopy after age 40.
- Fitness Test:
- Grip strength
- VO2 Max (Once per year)
- Centenarian decathlon age-adjusted challenges.
- Other Tests:
- Oral glucose tolerance test (OGTT)
- Continuous Glucose Monitor (CGM)
- “(You have a better chance of spotting this level of damage if using a more advanced type of CT scan, called a CT angiogram, which I much prefer to a garden-variety calcium scan[*4] because it can also identify the noncalcified or “soft” plaque that precedes calcification.)”
- Drugs
- Statins
- Metformin
- Rapamycin
Appendix
Other Ressources
Read This Next
- Get To Good Enough & Move On
- What I Learned from Tracking my Mood for 1000 days
- Peter Attia’s Nutritional Framework
- My 10-day Vipassana Silent Retreat Experience
- The Do-Nothing Morning Routine Experiment
- The Biometrics of High School Teaching
- Life Score: A Subjectively Objective Way to Evaluate your Life
- Atomic Habits – Book Notes
- How Emotions Are Made – Book Notes
- Four Thousand Weeks – Book Notes
- The Illustrated Happiness Trap – Book Notes
Affiliate Links
- Outlive – Peter Attia
- Becoming a Supple Leopard – Dr. Kelly Starrett
- I Don’t Want to Talk about it – Terrence Real
- Alaska Bear Sleep Mask
- How Emotions Are Made – Lisa Feldman Barrett
- Daylio app
- Tao Te Ching – Lao Tzu (Translated by Stephen Mitchell)
- Walking – Erling Kagge
- Silence – Erling Kagge
- Atomic Habits – James Clear
- Stillness is the Key – Ryan Holiday